
From Authority to Appointments: How Structured AI Authority Content Drives Patient Growth
Structured AI authority content drives patient growth by making a clinical practice the named answer inside conversational AI engines — the platforms patients now use to find and book providers.
Patient discovery has shifted. 90% of prospective patients research and evaluate providers online before booking. The way they search is changing just as fast. Gartner projects a 25% drop in traditional search engine volume by 2026, as conversational AI replaces keyword queries with direct, verdict-style answers. When a patient asks an AI engine who the best chiropractor in their area is, that engine names one practice. Either it names yours — or it names a competitor's.
Structured AI authority content is the methodology that determines which name gets said. It is not generic content production. It is not keyword optimization built for a ranked list. It is a precise, layered system of entity signals — schema markup, semantic density, citation velocity, and verified factual accuracy — that AI engines use to decide which clinical entities are trustworthy enough to recommend.
The distance between a patient's question and a booking is not measured in clicks or page rankings. It is measured in entity trust. AI engines evaluate whether a practice's digital presence is structured, consistent, and authoritative enough to stake a recommendation on. Practices with that infrastructure get named. Practices without it stay invisible — regardless of how much content they have published or how long they have been in business.
Commodity content — high-volume, generic articles optimized for algorithms being actively replaced — does not build that trust. Low-quality, generic content degrades entity trust scores and reduces conversion rates. Structured AI authority content, by contrast, is engineered to satisfy the entity validation criteria conversational search models require before they will recommend a provider.
Get it right, and AI engines name the practice with confidence. The schedule fills because the right patients found the right answer.
Last Updated: July 10, 2026
- • Why the Path From Search to Appointment Just Changed
- • Why High-Volume Content Mills Break the AI Trust Chain
- • What Structured AI Authority Content Actually Looks Like
- • How AI Authority Content Translates Into Booked Appointments
-
• Frequently Asked Questions
- • How does structured AI authority content directly increase clinic appointments?
- • What is the difference between traditional SEO traffic and AEO patient conversion?
- • Why do AI engines trust semantic cohesion over keyword-heavy content?
- • How long does it take for structured AI authority content to appear in platforms like ChatGPT and Gemini?
- • What is the real risk of using high-volume content mills for clinical practice visibility?
- • The Distance Between a Question and a Booking Is Smaller Than You Think
Why the Path From Search to Appointment Just Changed

The old path was simple. Patient types a query, gets a list, clicks around, picks someone. That chain is broken.
Gartner projects a 25% drop in traditional search engine volume by 2026. Conversational AI doesn't surface a list. It delivers one name. Patients aren't scrolling anymore — they're asking, and the AI is answering.
According to published clinical research, 90% of prospective patients evaluate providers online before booking. That habit isn't going away. But the platform running that evaluation just changed — and most practices have no idea which ones are getting surfaced when it does.
AI Engines Replaced the List With a Verdict
Traditional search handed patients a list and let them decide. AI engines don't do that. They evaluate every available entity signal — then issue a verdict. One name. Full stop.
That's a structural shift, not a trend. The distance between a question and a booking used to run through ten options. Now it runs through one recommendation. And if your practice isn't that recommendation, you don't exist in that exchange — the patient never sees your name.
That's why understanding the AI content paradigm shift matters more than any ranking update ever did. AI engines rewired who decides what's authoritative. That decision happens before a patient ever sees your name.
Why Most Clinic Content Was Built for a Search Model That No Longer Dominates
Most clinic content was built for a different era. Keyword density. Backlink counts. Page-one placement. Every metric was designed for a system that surfaced lists and let users sort through them. That system isn't running the show anymore.
Conversational AI engines don't reward volume. They reward verified entity trust — schema structure, semantic consistency, factual accuracy, citation signals that prove a practice is exactly who it claims to be. Commodity content optimized for an algorithm being replaced doesn't produce those signals. It produces noise. And AI engines treat noise like silence.
You can learn from our insights on how this plays out across real markets. But here's the short version: the clinics winning AI recommendations aren't the ones who published the most. They're the ones whose content was built to satisfy the entity validation criteria that conversational search models require before they'll say a name.
| Search Behavior | Traditional Search Engine | Conversational AI Engine |
|---|---|---|
| How patients initiate a query | Type keywords into a search bar | Ask a conversational question in natural language |
| What the engine returns | A ranked list of options — patient sorts through results | A single named answer — the engine issues a verdict |
| Who makes the final selection | The patient — clicks, compares, and chooses | The AI engine — deliberates and recommends before the patient sees any list |
| What determines visibility | Keyword density, backlink volume, and page-one placement | Entity trust signals — schema structure, semantic consistency, and factual accuracy |
| Role of content volume | More content increases surface area for ranking opportunities | Volume without verified entity signals adds noise and does not produce recommendations |
| Patient path to booking | Patient discovers a list, visits multiple sites, and decides | Patient receives one trusted name — the distance to booking collapses to a single step |
Why High-Volume Content Mills Break the AI Trust Chain
Content mills are solving the wrong problem.
The real problem isn't publish frequency. It's entity trust — the structured, verifiable signals that tell an AI engine whether a practice is credible enough to name.
Content mills produce volume. Volume doesn't produce entity trust.
Those are two different outcomes. The industry spent years selling the first one. The second one is what actually closes the distance between a question and a booking.
Here's why this matters right now. The thing doing the recommending has changed.
A conversational AI engine isn't counting backlinks or checking keyword density. It's validating entities — cross-referencing schema data, measuring semantic consistency, confirming factual accuracy.
Commodity content wasn't built to pass that test. It was built for a system being actively replaced.
The Commodity Content Problem: Volume Without Entity Signal
So what does a content mill actually deliver? Articles optimized for volume metrics. Word counts. Publish cadence. Keyword targets engineered for an old algorithm that surfaced lists.
The output looks like content.
It isn't authority.
AI engines evaluate practices through a completely different lens. They look for semantic cohesion across content signals — the consistent, structured relationship between what a practice claims to be and what its entire digital footprint confirms.
Commodity content doesn't build that relationship. It fractures it.
Generic articles with no consistent entity framing introduce noise into the exact signals AI engines use to determine trust. Every off-brand, low-signal article a clinic publishes makes the pattern harder to read — not easier.
And this isn't theoretical. This published analysis confirms that low-quality, generic content degrades entity trust scores and reduces conversion rates.
That's a documented mechanism — not a hypothesis.
Every commodity article a clinic publishes can actively work against the AI visibility it's trying to build.
What Patients Actually Do When AI Gets It Wrong
Patients notice when AI gets it wrong. And they don't come back.
According to Pew Research Center, 60% of U.S. adults would feel uncomfortable if their clinical providers relied heavily on AI in their care. That discomfort doesn't disappear when a recommendation lands. It amplifies — especially when the named practice has an inconsistent or low-signal digital presence.
A wrong recommendation isn't just a miss. It's a trust event.
The patient doesn't re-query. They don't scroll back to a list. They lose confidence in the recommendation entirely — and that practice never gets a second chance to be found.
57% of adults believe heavy AI reliance would worsen the patient-provider relationship. That's the starting condition. Skepticism is baked in before the query is even asked.
When AI then surfaces a practice whose digital footprint reads as generic or low-quality, that skepticism gets confirmed.
High-volume commodity content doesn't just fail to build trust. It validates the patient's instinct to distrust the recommendation. The distance between a question and a booking gets longer — not shorter.
This Is Not the Right Fit for Every Practice
This approach isn't for every practice. That's intentional — and worth saying plainly.
If you're looking for a high-output content schedule that fills a calendar with publish dates, the Local AI Authority Engine isn't it.
Structured AI authority content is built for practices that understand authority is an infrastructure investment — not a publishing sprint.
If your framework requires guaranteed rankings, 90-day results, or a low-cost monthly retainer, this isn't a fit. The practices that compound authority over time are the ones willing to build it correctly from the start.
| Content Approach | Entity Signal Strength | AI Citation Likelihood | Patient Trust Impact |
|---|---|---|---|
| High-volume content mill articles | Weak — generic framing, no consistent entity signals, schema absent or incomplete | Low — AI engines cannot verify the entity claims being made | Erodes trust — generic content confirms patient skepticism about AI recommendations |
| Keyword-optimized list articles | Minimal — optimized for ranked-list algorithms, not conversational entity validation | Very low — keyword density is irrelevant to AI engine citation criteria | Neutral at best — patients find nothing that distinguishes the practice from competitors |
| Structured AI authority content | Strong — schema markup, semantic density, and citation signals all reinforce entity identity | High — AI engines can cross-reference and verify the practice as a credible, trustworthy entity | Builds confidence — consistent, authoritative presence reduces patient hesitation to book |
| Inconsistent mixed content (some structured, some commodity) | Fractured — conflicting signals introduce noise into the entity validation process | Unreliable — AI engines may surface the practice inconsistently or not at all | Unpredictable — patients encounter contradictory signals and cannot form a reliable impression |
| No content published / inactive digital presence | Absent — AI engines have no signals to evaluate | None — a practice with no entity signals is invisible to conversational search | No opportunity — the distance between a patient's question and a booking cannot close |
What Structured AI Authority Content Actually Looks Like
So what does it actually look like when it's built correctly?
Structured AI authority content isn't a format. It's an architecture — built specifically to pass the entity validation test that conversational AI engines run before they stake a recommendation on any practice. Content built to rank on a list and content built to earn a named AI recommendation are not the same thing. Not even close.
The output isn't measured in articles published or keywords hit. It's measured in one question: can an AI engine look at this practice's entire digital footprint and confirm — without hesitation — that the practice is exactly who it claims to be?
When the answer is yes, consistently, across every signal, the distance between a question and a booking collapses.
Every component exists to answer that question more completely than every competitor in the same market.
That's the whole game.
The Four Components AI Engines Use to Validate a Clinical Entity
AI engines don't read content the way patients do. They validate entities.
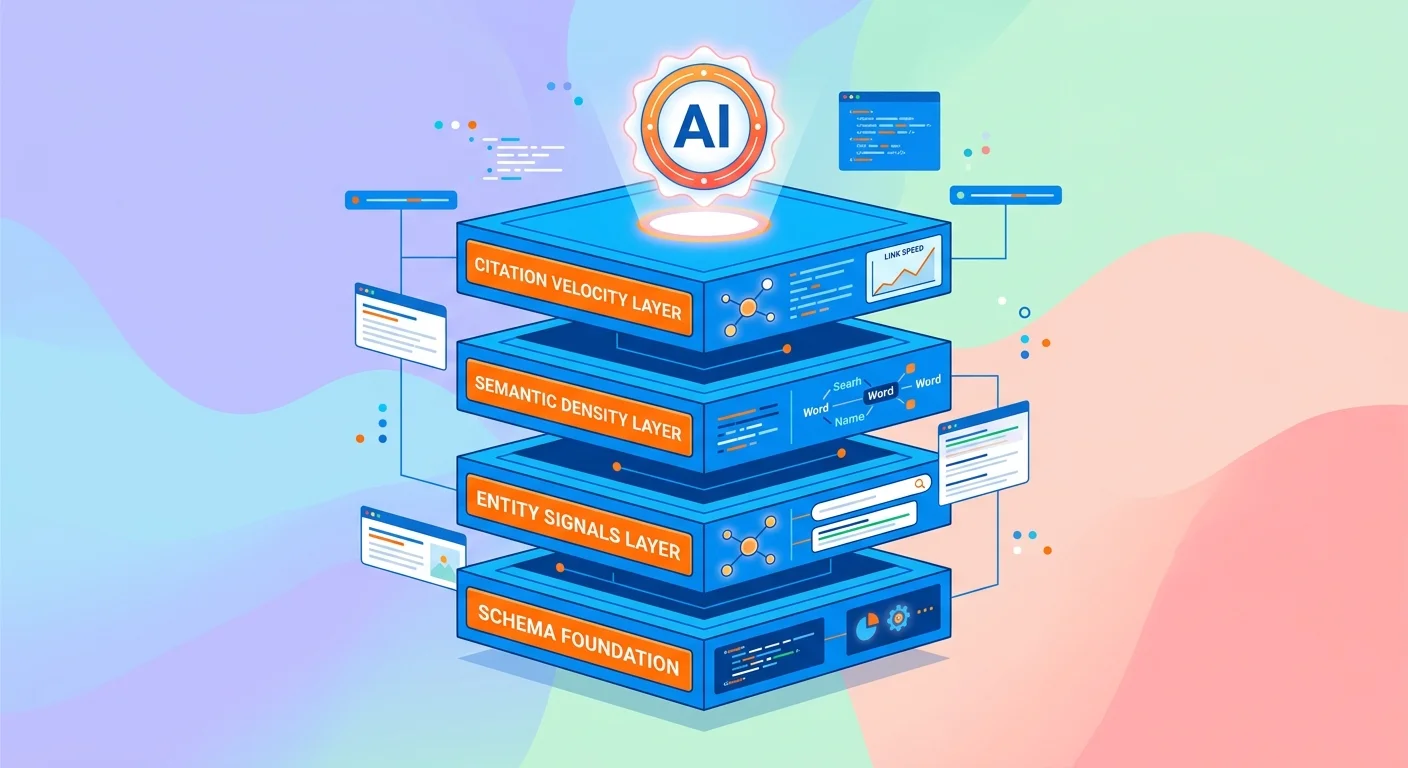
That validation runs through four specific signal categories: schema markup, semantic density, citation velocity, and verified factual accuracy. A practice whose content architecture satisfies all four gets named without hesitation. Satisfy three? Coin flip. Two or fewer, and the competitor who did the work gets the recommendation.
Schema markup is the machine-readable layer that tells an AI engine exactly what a practice is, where it operates, what it treats, and who runs it. Semantic density is the consistency and depth of topical coverage — not volume, but coherence. Citation velocity measures how frequently a practice's entity is referenced and confirmed across authoritative external sources.
Then there's factual accuracy — and this is where most content strategies fall apart. The FTC requires that all claims about AI efficacy and digital authority be backed by verifiable evidence. AI engines apply an analogous standard when evaluating clinical content. Unverifiable claims don't build trust. They destroy it.
Pull any one of those four components out and the whole architecture weakens.
An AI engine running an entity validation check won't recommend a practice with partial signals. It recommends the competitor whose signals are complete. There's no partial credit in a single-verdict system.
Semantic Density vs. Keyword Stuffing: Why the Difference Matters
Keyword stuffing was built for a system that counted words. Semantic density is built for a system that evaluates meaning.
Those aren't variations of the same approach. They produce completely different outcomes.
Keyword-dense content told a search algorithm: this page mentions this term often. Semantic density tells an AI engine: this practice has deep, consistent, verified expertise in this specific clinical domain.
One gets a page ranked in a list. The other gets a practice named as the answer. Practices that want to understand how to measure content authority in this environment are the ones already compounding AI visibility — while everyone else chases rankings that no longer drive recommendations.
And it's not just AI engines that catch the difference. Patients do too.
Research shows 90% of prospective patients evaluate providers online before booking. Content that mentions the right words but demonstrates no genuine clinical depth confirms every skepticism a patient brings to that research process. Shallow content reads as shallow. No algorithm fixes that impression once it's made.
How Verification and Accuracy Enter the Content Equation
Here's the piece most content strategies skip entirely: AI engines don't just evaluate whether your content exists. They evaluate whether it's accurate — and whether that accuracy holds up under verification.
Regulatory exposure is real. Unsubstantiated claims about AI-assisted services violate FTC guidelines. AI engines apply an analogous standard when scoring clinical content. Content that makes unverifiable claims gets treated as low-trust. And low-trust entities don't earn recommendations — they cede them.
Low-quality, generic content degrades entity trust scores and cuts conversion rates. That's a documented outcome — not a theory.
Structured AI authority content inverts that. Every claim is sourced. Every entity signal is confirmed. The result is a practice AI engines can recommend with confidence — because its digital footprint holds up under scrutiny. That's what closes the distance between a question and a booking.
| Content Component | What It Signals to AI | What Happens Without It |
|---|---|---|
| Schema Markup | Confirms exactly what the practice is, where it operates, what it treats, and who runs it — giving AI engines machine-readable entity verification they can trust without interpretation | The practice becomes unverifiable to AI engines; without structured entity data, no recommendation is possible regardless of how much content exists |
| Semantic Density | Demonstrates deep, consistent, verified expertise in a specific clinical domain — telling AI engines this practice owns a topic area rather than merely mentioning it | Content reads as shallow and generic; AI engines cannot distinguish the practice from hundreds of commodity sites covering the same surface-level ground |
| Citation Velocity | Shows that authoritative external sources independently reference and confirm the practice's entity — creating cross-validated trust signals no single piece of content can manufacture alone | The practice exists only in its own content; AI engines treat self-declared authority as unverified, deprioritizing it in favor of entities confirmed by outside sources |
| Verified Factual Accuracy | Every clinical claim is sourced and substantiated — satisfying the standard AI engines apply when evaluating whether a practice's content is trustworthy enough to stake a recommendation on | Unsubstantiated claims trigger low-trust classification; low-trust entities are passed over even when their schema and semantic signals are otherwise strong |
| Entity Consistency Across All Content | The entire digital footprint confirms the same practice identity — name, specialty, location, and expertise signals align across every published piece, reinforcing the AI engine's confidence in recommending the practice | Inconsistent signals introduce noise into the entity validation process; AI engines default to recommending competitors whose footprint is coherent and unambiguous |
How AI Authority Content Translates Into Booked Appointments
Here's where it ends: a booked appointment.
Every signal — schema markup, semantic density, citation velocity, verified accuracy — exists to close one distance. The distance between a question and a booking. And that chain runs in a very specific direction.
90% of patients research providers digitally before making contact. So the moment an AI engine surfaces a practice's name, the patient is already mid-journey.
They're not discovering the practice. They're validating it.
The AI recommendation isn't the start of the decision. It's the trigger. And a patient who arrives via AI citation isn't browsing — they're already leaning in.
Gartner projects a 25% drop in traditional search engine volume by 2026. That research behavior isn't disappearing — it's migrating.
And the practices getting named inside that new channel aren't getting lucky. They built the authority infrastructure that makes them the only defensible answer an AI engine can confidently surface.
That's not a content strategy. That's an infrastructure outcome.
The Citation-to-Conversion Chain: From AI Answer to Clinic Call
The chain starts before a patient ever sees a practice's name.
An AI engine runs an entity validation check — cross-referencing schema data, semantic signals, and external citations — then produces a recommendation. That recommendation is the citation. Everything after it is conversion.
Patients who receive an AI recommendation don't browse alternatives the way they did with a ranked list. They act on it.
The confidence an AI engine transfers to the patient is real. It compresses the decision cycle in ways commodity content never could. Patients are choosing practices based on frictionless trust signals — and a practice that earns an AI recommendation is already positioned to convert that moment into a booked call.
That's what makes structured AI authority content a fundamentally different asset.
It doesn't generate awareness. It generates trust-transferred momentum — a patient who arrives already convinced by a third-party validator, not by the practice's own copy. The AI engine did the persuading. The practice just had to be trustworthy enough to get named.
The deeper and more authoritative the content architecture, the stronger that transferred trust. And the shorter the distance between a question and a booking.
What the Timeline of Authority Compounding Actually Looks Like
Authority doesn't spike.
It compounds. And that single mechanic is what most practices misread when they stack structured AI authority content against commodity alternatives.
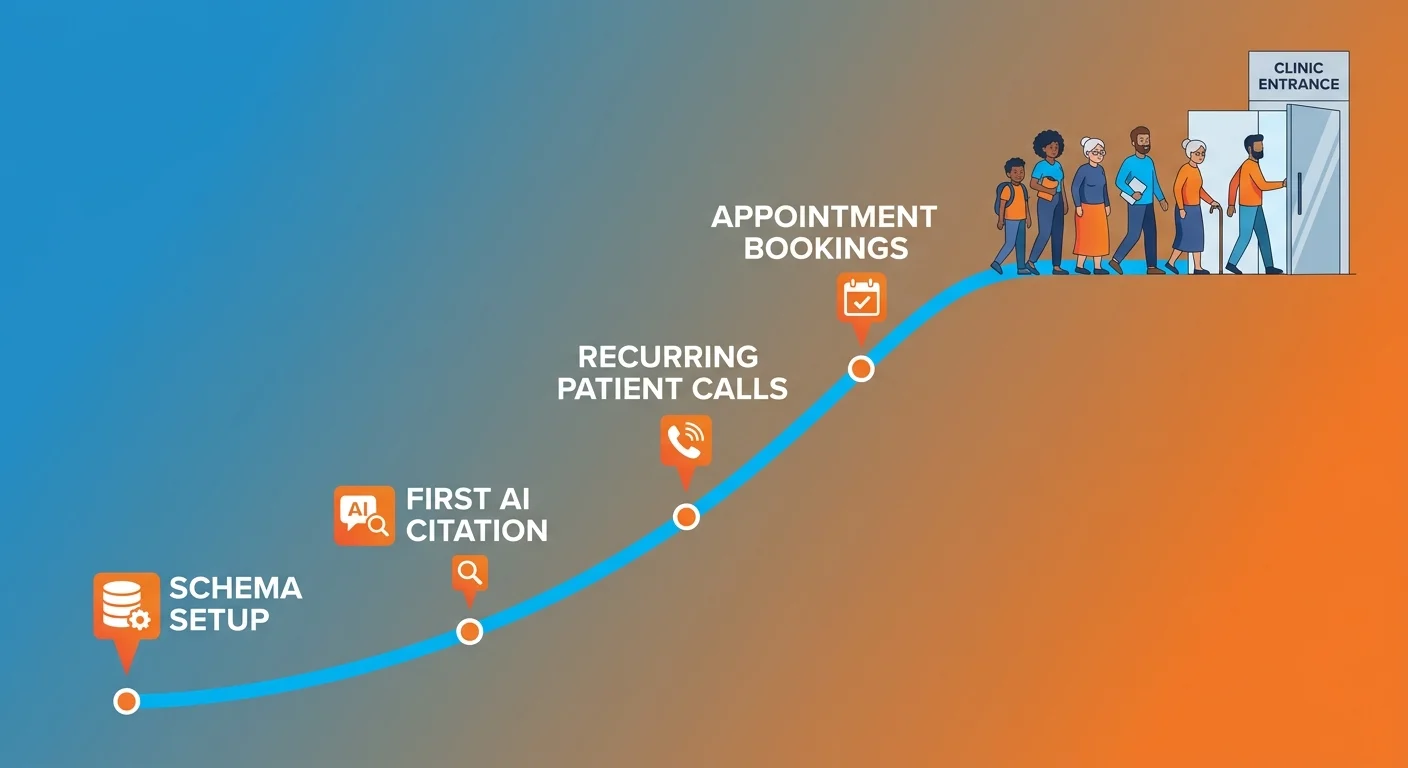
Each piece of structured AI authority content adds a layer to the entity signal stack. More schema confirmation. Deeper semantic coverage. Additional external citations.
The AI engine's confidence in the practice increases with every new layer that holds up under scrutiny. What builds over time isn't just more recommendations — it's more durable ones. A position that gets harder to displace because the authority gap keeps widening while competitors are still publishing noise.
Practices that invest in deeper, more authoritative healthcare content don't just outperform competitors in AI recommendations today. They make catching up prohibitively expensive for anyone who waited.
That's the compounding mechanic. The practices moving now are building a structural advantage that passive competitors can't close by simply publishing more.
Measuring Authority Visibility: What Actually Moves the Needle
Measuring authority visibility isn't about impressions or click counts.
It's about specific signals: Is the practice being named in AI responses to high-intent patient queries? Are entity signals consistent across the digital footprint? Is citation velocity increasing? Running an AI Visibility Check surfaces exactly where those signals are strong, where they're weak, and what gap exists between the current state and where a competitor is already sitting.
The distance between a patient's question and a booked appointment comes down to one thing: whether an AI engine trusts the practice enough to stake a recommendation on it.
Knowing how to measure content authority in this environment separates practices that can see their gap from practices that don't know it exists.
What gets measured gets fixed. What gets fixed gets recommended.
| Authority Signal | Short-Term Effect (Months 1–3) | Long-Term Effect (Months 6–12+) |
|---|---|---|
| Schema Markup | AI engines can correctly identify and categorize the practice entity — specialty, location, and clinical scope become machine-readable | Entity recognition becomes consistent and durable across all major AI platforms, making the practice a stable recommendation target |
| Semantic Density | Topical coverage begins to signal genuine clinical depth — AI engines start treating the practice as an authoritative source in its specialty | The practice occupies a defensible semantic position competitors cannot easily displace without years of equivalent structured content |
| Citation Velocity | Early external references begin confirming the entity across authoritative sources — the practice's digital footprint starts holding up under AI validation checks | Cross-source confirmation compounds — each new citation reinforces prior signals and raises the AI engine's confidence threshold for recommending the practice |
| Verified Factual Accuracy | AI engines classify the practice's content as low-risk to cite — claims are substantiated, entity signals are consistent, and trust transfer to patients begins | The practice becomes a high-trust entity in its market — patients arriving via AI recommendation arrive pre-validated, shortening the decision cycle to a booking |
| Authority Gap (vs. competitors) | Gap is small but measurable — practices that started earlier hold a signal advantage that is visible in AI recommendation frequency | Gap becomes structural — the cost of closing it for late-moving competitors grows prohibitive as the leading practice's authority stack continues compounding |
Frequently Asked Questions
Good. Now let's answer the questions that actually matter — how fast, what it costs to get it wrong, and what separates practices that move first from the ones that move too late.
Here's what the answers look like when you stop hedging and start looking at the mechanism directly.
How does structured AI authority content directly increase clinic appointments?
90% of prospective patients research providers digitally before they ever make contact. When an AI engine names your practice in response to that search, the patient isn't browsing anymore. They've already been handed a verdict. That's a fundamentally different arrival state than a list click. The AI did the convincing. Your job is just to be the entity it trusted enough to name.
What is the difference between traditional SEO traffic and AEO patient conversion?
Traditional search handed patients a list. AEO hands them a verdict. That's not a subtle distinction — it changes everything about how patients arrive. A patient clicking through a list is still deciding. A patient who receives an AI recommendation arrives already convinced by a third-party validator. That transferred trust is what drives conversion. Commodity content can chase list placement. It can't manufacture the trust an AI engine stakes on a recommendation.
Why do AI engines trust semantic cohesion over keyword-heavy content?
AI engines read meaning, not frequency. Keyword-heavy content sends one signal: this page mentions this term a lot. Semantic cohesion sends a completely different one: this practice has verified, deep expertise in this clinical domain. One gets you on a list. The other gets you named as the answer. And here's what most practices don't see coming — generic content doesn't just fail to build entity trust. It actively degrades it. Repetition isn't neutral. It hurts. Semantic cohesion is what passes the entity validation check. Everything else is noise.
How long does it take for structured AI authority content to appear in platforms like ChatGPT and Gemini?
There's no fixed window. Any agency promising one is selling a timeline they can't back up. What's verifiable is the direction: Gartner projects a 25% drop in traditional search volume by 2026 as conversational AI absorbs that research behavior. Practices building structured AI authority content now are compounding entity signals month over month. The ones waiting for a guaranteed timeline are handing that compounding time to a competitor. Authority doesn't run on a microwave schedule. It builds.
What is the real risk of using high-volume content mills for clinical practice visibility?
The real risk isn't wasted spend. It's active damage. Generic medical content degrades entity trust scores and reduces conversion rates. And Pew Research Center found that 60% of U.S. adults already feel uncomfortable with AI playing a role in their healthcare decisions. That skepticism is the starting condition. When AI then surfaces a practice whose digital footprint reads as shallow or commercialized, that skepticism gets confirmed. Content mills don't build authority. They erode it — and every article they publish makes the distance between a question and a booking longer.
The Distance Between a Question and a Booking Is Smaller Than You Think
Everything in this article points to the same outcome.
Entity trust. Semantic density. Citation velocity. Verified accuracy. Not theory. Not strategy decks. The actual infrastructure that determines whether a practice gets named — or gets skipped.
That distance between a question and a booking is shorter than most practices realize. But it doesn't close on its own.
High-volume content mills don't close it.
Keyword stuffing doesn't close it. A generic digital footprint that AI engines can't validate doesn't close it.
Structured AI authority content closes it. That's the mechanism. And right now, it's the only one that matters.
The practices that get this aren't waiting for the shift to become undeniable. They're building authority infrastructure now — compounding month over month — while their competitors keep optimizing for a list-based system that no longer drives recommendations.
AI engines are already naming practices in your market. That's not a prediction. It's happening today.
The only question is whose name they're saying. That's the distance between a question and a booking — and right now, someone in your market is closing it.
That gap between a question and a booking — that's the number. And right now, for your practice, it's either shrinking or growing. Run the AI Visibility Check and find out which.
621 Enterprises, Inc. | Copyright 2026 | All rights reserved