
Beyond Volume: How AI Authority Content Creates Deeper, More Authoritative Healthcare Content
AI authority content in healthcare is not a volume game. It is a verification game.
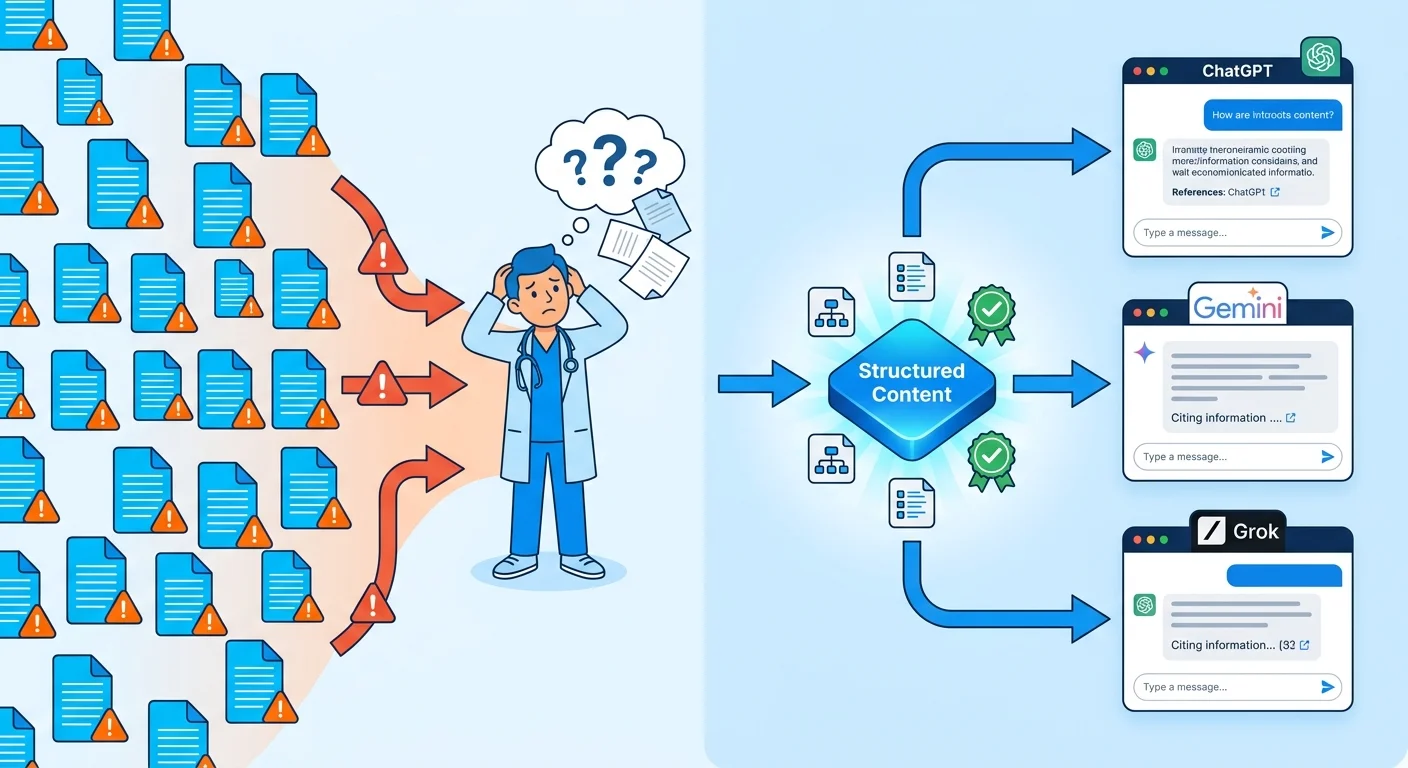
The practices AI engines recommend and the ones that stay invisible are separated by one variable: whether their content is structured, sourced, and validated at a depth that answer engines can actually trust.
ChatGPT, Gemini, and Perplexity do not operate like traditional search. Publishing frequency is not rewarded. Entity credibility is. A practice that publishes fifty thin articles has not built authority. It has built noise.
Healthcare raises the stakes considerably. Peer-reviewed research published through the National Institutes of Health documents that generative AI tools produce dangerous omissions in medical information when verified knowledge structures are absent. The World Health Organization issued explicit governance guidelines requiring hallucination safeguards specifically because medical misinformation causes direct patient harm. The FTC requires pre-existing scientific proof behind any AI-related healthcare marketing claim. The Department of Health and Human Services finalized the HTI-1 rule establishing transparency requirements for AI algorithms used in clinical decision support.
That is the environment a medical practice is trying to build visibility inside. Regulatory pressure from every direction. AI engines designed to penalize inaccuracy. Patients whose health decisions depend on what those engines say.
AI authority content — built correctly — satisfies both the technical and compliance demands at once. It establishes Entity Trust by structuring clinical information in formats AI engines are designed to extract and cite. It builds Citation Velocity by adding verified, schema-supported content that compounds over time.
AI says your name or it doesn't. Everything else is just content.
Last Updated: July 10, 2026
- • Why Volume Fails Healthcare Practices in the Age of AI
- • What Entity Trust Actually Looks Like in Healthcare Content
- • How Citation Velocity and Semantic Density Compound Over Time
- • Regulatory Stakes and the Clinical Accuracy Standard
- • Patient Trust, AI Recommendations, and the Visibility Gap
-
• Frequently Asked Questions
- • Why does traditional healthcare SEO fail to rank your clinical voice in AI searches?
- • Is AI Authority content safe from HIPAA and regulatory healthcare penalties?
- • How does iTech Valet build Entity Trust for medical practices compared to standard SEO?
- • What are the clinical risks of using high-volume commodity content mills?
- • How long does a clinic take to build enough Citation Velocity to dominate ChatGPT and Gemini?
- • What is the difference between Semantic Density and keyword density in healthcare content?
- • The Verdict on Volume
Why Volume Fails Healthcare Practices in the Age of AI
Volume worked when the game was keyword rankings. Publish enough, optimize enough, get on the list somewhere. That chain is broken. And healthcare practices still playing that game aren't just behind — they're invisible where it counts.
ChatGPT, Gemini, and Perplexity don't return a list. They return a verdict. They evaluate entity credibility. Not publishing frequency. A practice flooding the web with generic articles hasn't built authority. It has built a signal AI engines are designed to ignore.
And in healthcare, the cost isn't just visibility. It's credibility. Pew Research Center found that 60% of U.S. adults already feel uncomfortable with their healthcare providers relying on AI for clinical care. When the content those engines surface is thin, unverified, and clinically shallow, that discomfort compounds fast. The practice doesn't just lose the recommendation. It loses the trust that makes the recommendation worth having.
The Shift From Search Lists to AI Verdicts
Traditional SEO optimized for a list. AI search produces a verdict. Those aren't variations of the same thing. Treating them like they are is exactly why most medical practices are invisible right now.
But here's the thing — this isn't a cosmetic update to your content calendar. What content is supposed to do has fundamentally changed. The practices that understood this content paradigm shift in healthcare early are the ones AI engines cite when patients ask who to trust. The ones still publishing keyword-stuffed posts? They're building noise. And answer engines filter that noise out before they ever form a response.
Why High-Volume Content Mills Break Clinical Authority
So what do high-volume content mills actually do to a medical practice's AI authority? They don't just fail to build it. They burn it down.
National Institutes of Health peer-reviewed research documents that generative AI tools create dangerous omissions in healthcare information unless integrated into verified knowledge structures. Commodity content mills produce exactly the kind of unverified, generically structured text AI engines are built to distrust. Every thin article published under a practice's name is a signal. Not of authority — of its absence.
Clinical authority isn't built by publishing more. It's built by publishing verifiably. Structured, sourced, schema-supported content tells AI engines something a hundred keyword-optimized posts never will: that this practice understands its subject at a depth worth citing. That's the line between being the verdict and being the noise.
| Content Approach | How Search Engines Processed It | How AI Answer Engines Process It | Outcome for the Practice |
|---|---|---|---|
| High-frequency keyword blogging | Rewarded publishing volume and keyword density; page-one rankings achievable through consistent output | Filtered out as low-credibility noise; lacks the entity signals and structured validation AI engines require to form a citation | Practice publishes constantly, ranks on a list fewer patients consult, earns zero AI recommendations |
| Generic AI-generated content mills | Indexed and partially rewarded for fresh content signals and topical breadth | Identified as unverified, structurally thin, and clinically untrustworthy; actively deprioritized in answer formation | Practice builds surface-level web presence with no Entity Trust — invisible to ChatGPT, Gemini, and Perplexity |
| Repurposed or syndicated clinical content | Tolerated as supplementary content; occasionally rewarded for topical relevance | Treated as duplicate or derivative signal; insufficient to establish original clinical authority for the practice entity | Practice appears generic and interchangeable — AI engines cannot distinguish it from any other source citing the same material |
| Structured AEO authority articles | Rewarded for topical relevance, keyword inclusion, and internal linking structure | Recognized as a verified, schema-supported, entity-credible source; surfaces as a trusted citation when patients ask who to see | Practice earns AI recommendations — becomes the verdict, not one item on a list |
| Dual-AI validated clinical content | Treated identically to other well-structured content; no algorithmic distinction for validation methodology | Recognized at the highest trust tier — every claim sourced, every structure verifiable, every entity signal reinforced | Practice compounds authority over time; AI engines consistently name it as the authoritative answer in its market |
What Entity Trust Actually Looks Like in Healthcare Content

Entity Trust is not a content metric. It is a structural signal — the cumulative evidence AI engines use to decide whether a medical practice is worth citing at all.
Here's what most practices get wrong: ChatGPT, Gemini, and Perplexity don't evaluate how much content you've published. They evaluate how verifiable it is. Schema markup, consistent NAP data, clinically sourced claims, structured content hierarchies — those are the signals that tell an answer engine your practice understands its subject at a depth worth recommending. Publishing volume doesn't speak that language.
The HHS-ONC's published policy framework made this concrete. The HTI-1 rule locked in strict transparency metrics for predictive AI algorithms used in clinical decision support. That regulatory posture doesn't stay in government documents. It filters directly into how answer engines evaluate medical content. Practices whose content lacks verifiable depth don't just rank poorly. They get excluded from the trust architecture entirely.
The Three Structural Signals AI Engines Verify
Here's the first check: consistent entity data. Does your business name, address, phone number, and clinical specialty align across every platform, directory, and content source? One mismatch isn't a minor gap. It's a disqualification signal.
Second check: semantic density. Does the content show genuine clinical depth, or is it skimming surface topics with generic language? Research indexed through the National Institutes of Health confirms that generative AI tools produce omissions in healthcare information when verified knowledge structures aren't in place. Thin content doesn't just fail that test. It actively registers as a liability inside the engine's trust evaluation.
Third check: schema integrity. Is the content structured so AI engines can extract, parse, and validate it without ambiguity? A practice that publishes well-sourced clinical information without schema support is handing a well-written document to a reader who can't open the file. Structure is not optional. It's the delivery mechanism. Without it, accuracy doesn't matter — the engine never reaches it.
How Entity Trust Is Built for Medical Practices
Building Entity Trust means engineering all three signals at once. Not sequentially. Entity data, semantic density, and schema integrity compound together. Fix one while neglecting the others and the authority signal stays incomplete — and an incomplete signal reads the same as no signal at all.
That's why understanding how AI authority content amplifies your clinical voice matters before you publish another word. It's not just what gets published. It's how the content is architected to speak directly to the validation logic AI engines apply. Every article, every schema tag, every consistent entity signal is a brick. The engine either trusts the structure or dismisses it.
The practices that build this correctly don't win because they published more. They win because every piece of content they publish adds a verifiable layer to an authority infrastructure AI engines are designed to recognize. That's the line between a medical practice that gets cited and one that doesn't exist in the answer at all.
| Entity Signal | What AI Engines Check | What a Content Mill Delivers | What AI Authority Content Delivers |
|---|---|---|---|
| Entity Data Consistency | Does the practice name, address, phone, and specialty align identically across every platform, directory, and content source? | Generic content with no structured NAP enforcement — entity signals scatter across platforms and contradict each other | Consistent, structured entity data embedded across every article, directory listing, and schema tag — no ambiguity for the engine to resolve |
| Semantic Density | Does the content demonstrate genuine clinical depth, or does it skim surface topics with generic, interchangeable language? | Surface-level keyword coverage that reads as authoritative but contains no verifiable clinical specificity | Clinically sourced, specialty-specific content structured to demonstrate subject-matter depth AI engines are designed to recognize |
| Schema Integrity | Is the content structured so AI engines can extract, parse, and validate it without ambiguity? | Unstructured text blocks with no schema markup — well-written documents that answer engines cannot open or trust | Schema-supported content architecture that gives AI engines a clear, machine-readable map of what the practice is and what it knows |
| Citation Traceability | Are clinical claims tied to verifiable, institutional sources that answer engines can cross-reference? | Unsourced or loosely attributed claims that AI engines flag as unverifiable — a liability signal, not an authority signal | Every clinical claim anchored to peer-reviewed or institutional sources, giving AI engines the verification trail they require before citing |
| Content Hierarchy | Does the practice's content architecture reflect a coherent, topically authoritative structure — or a flat pile of disconnected posts? | Disconnected, volume-driven articles with no internal linking strategy — no compounding authority signal for AI engines to follow | Structured content hierarchies with intentional internal linking that build topical authority across every article published |
How Citation Velocity and Semantic Density Compound Over Time
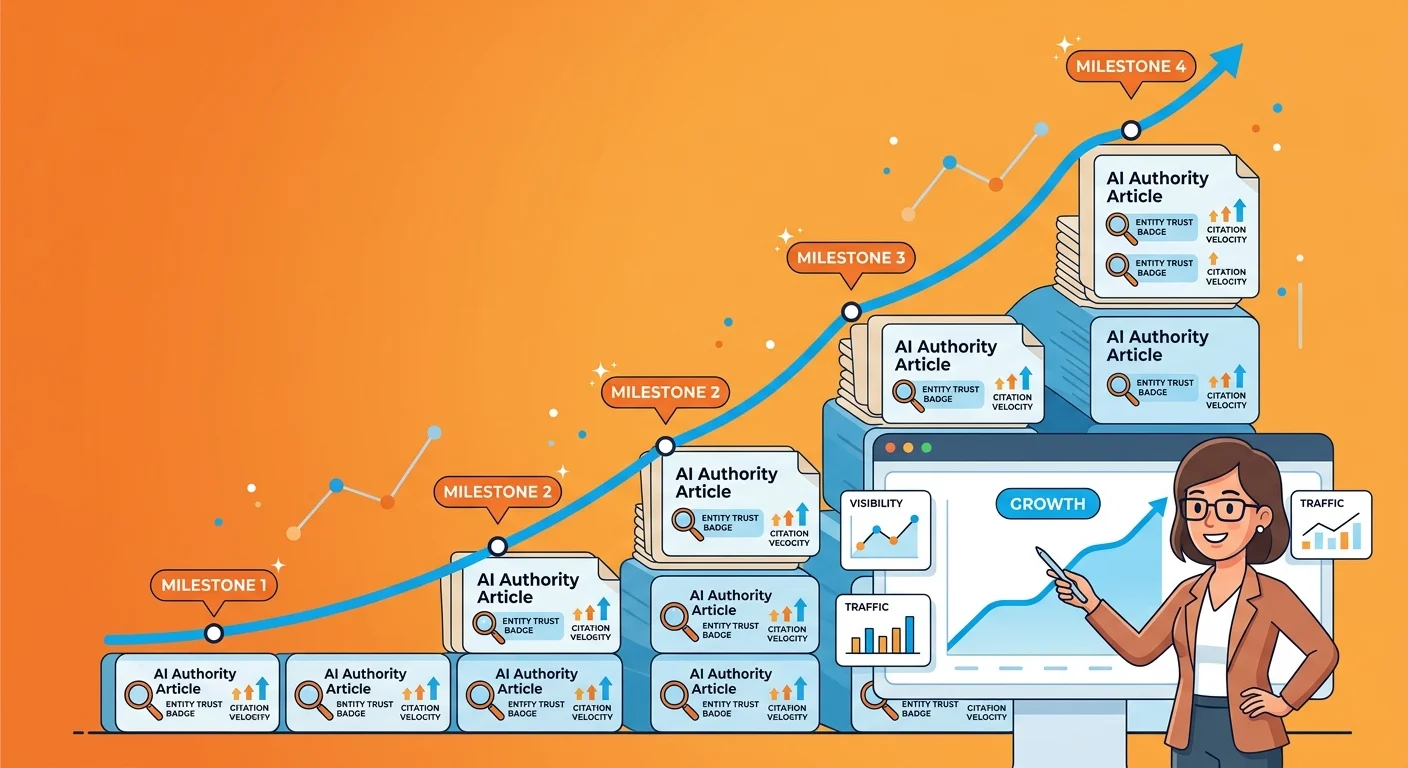
Citation Velocity isn't about how fast you publish. It's about how consistently verified, structured, clinically sourced content accumulates into a signal AI engines can actually trust.
Speed without verification builds noise. Cadence with verification builds authority.
Every AI authority article a practice publishes is a new data point in that signal. Not a standalone post. Not a keyword hit. A verifiable claim, properly structured, that adds one more layer to the cumulative picture of a practice worth citing.
The WHO's governance guidelines on AI in healthcare exist for a reason: unverified medical content causes real patient harm. Answer engines are built to enforce that standard before they surface a recommendation. Every article you publish either earns credibility inside that system — or registers as a liability.
Semantic Density works the same way — but it cuts in both directions. Every article that demonstrates genuine clinical depth sharpens the semantic fingerprint AI engines use to classify a practice as authoritative.
Thin content blurs that fingerprint. Verified, structured content sharpens it. And the gap between the practice publishing verified content and the one publishing generic volume widens with every article either of them puts out. That gap doesn't stay still. It accelerates.
Why Each AI Authority Article Builds on the Last
Here's the thing about compounding authority: the second article is easier to trust than the first. The tenth is easier to trust than the second.
AI engines don't grade each article in isolation. They evaluate the entire content architecture as a unified body of evidence.
When each article links to prior articles, reinforces consistent entity signals, and builds on established clinical claims, the authority infrastructure gets stronger with every addition. That's Citation Velocity in practice — not a race to publish, but a disciplined cadence of verified content that gives AI engines more reasons, month over month, to treat a practice as the definitive source.
For practices thinking through the compliance implications of this approach, structural rigor isn't a liability. It's the exact thing that keeps a practice on the right side of regulatory scrutiny.
McKinsey's research on generative AI in healthcare is direct: the entire value proposition depends on factual correctness as its foundation. That isn't a content preference. It's the architecture.
A practice publishing verified, schema-supported articles builds something that gets more valuable with every addition. A practice publishing generic content builds something AI engines learn to ignore. And that downgrade compounds just as fast as the upgrade does. The direction you're moving is always accelerating — you just don't notice until the gap is already too wide to close quickly.
The Anti-Persona in Healthcare Content: Who This Is Not For
Here's the thing: not every medical practice belongs in this conversation. Being clear about that upfront is more useful than pretending otherwise.
If you're looking to flood the web with articles in the next thirty days to spike a traffic metric, this isn't that. AI authority content compounds over time. It's built in layers — structured entity signals first, verified clinical content on top, schema integrity reinforcing both.
If your decision framework requires measurable results before the foundation is even in place, this approach will frustrate you before it helps you. That's not a criticism. It means the timing isn't right.
And if you believe that volume alone — more articles, more keywords, more publishing frequency — is the lever that moves AI recommendations, the methodology here will feel unnecessarily slow.
It is designed for practices that want to be the name AI says. Not one of many names a generic search might surface. Those are different goals. This approach serves one of them.
| Month of Execution | Entity Signals Accumulated | AI Confidence Level | Competitive Outcome |
|---|---|---|---|
| Month 1–2 | Business name, address, phone, and specialty confirmed across core directories and platforms; initial schema markup deployed; first verified clinical articles published | Low — AI engines have detected the entity but lack sufficient cross-referenced signals to classify it as authoritative | Practice is largely invisible in AI-generated recommendations; competitors with established entity signals dominate responses |
| Month 3–4 | Consistent NAP data reinforced across additional platforms; semantic density deepens as published articles build on prior clinical claims; internal linking structure begins to form a coherent content architecture | Moderate — AI engines can cross-reference multiple verified signals and begin associating the practice with specific clinical specialties | Practice begins appearing in AI responses for narrowly defined queries; gap with top competitors narrows slightly but is not yet closed |
| Month 5–6 | Entity signals now consistent across all major platforms and directories; schema integrity reinforced across the full content library; clinical depth demonstrated across multiple topic clusters | Growing — AI engines classify the practice as a credible source for its defined specialty and begin surfacing it in response to broader clinical queries | Practice competes directly with established entities for AI recommendations; early-mover advantage begins to express itself in how often the practice is named as a primary answer |
| Month 7–9 | Verified clinical content compounds into a recognizable semantic fingerprint; prior articles cited and reinforced by newer ones; authority infrastructure functions as a unified, self-reinforcing body of evidence | High — AI engines treat the practice as a structurally verified, clinically credible source worthy of consistent citation across a broad range of relevant queries | Practice is routinely named as a top recommendation in its specialty and market; competitors without equivalent entity infrastructure lose ground with each passing month |
| Month 10–12+ | Full authority infrastructure in place — entity data, semantic density, and schema integrity operating in concert; each new article strengthens an already established foundation rather than building from scratch | Authoritative — AI engines default to this practice as the definitive source in its specialty; the compounding effect means each additional article yields increasing returns on authority | Practice is the AI-recommended answer for its market and specialty; the competitive gap is now structural and widens automatically as the authority infrastructure continues to grow |
Regulatory Stakes and the Clinical Accuracy Standard
Most practices treat AI visibility as a marketing problem. It isn't. It's a compliance problem — and most of them are already exposed.
The FTC enforcement guidance doesn't leave room for interpretation. Companies making AI-related healthcare marketing claims must have pre-existing scientific proof to support those claims — before anything goes live. Not as a best practice. As a compliance floor. And commodity content mills aren't built anywhere near it.
That's where the gap between generic publishing and AI authority content becomes a legal gap, not just a visibility one. Keyword-stuffed articles don't just fail to build Entity Trust. Every unsourced claim, every assertion without clinical grounding, sits under the practice's name as a liability. Volume-based publishing doesn't just underperform. It exposes.
What the FTC and HHS Expect From AI-Assisted Healthcare Content
The FTC has been explicit about the sequence. Scientific evidence must exist before the content publishes. Not after. Not eventually. Before. That standard applies to every AI-assisted healthcare marketing claim a practice puts into the world.
The HHS Office of the National Coordinator finalized the HTI-1 rule with the same intent — strict transparency metrics for predictive AI algorithms in clinical decision support. Two agencies. Same direction. And the FTC made the enforcement logic identical: scientific proof before publication, not after. Neither one is asking nicely. In healthcare, AI-assisted content is held to a factual standard no other industry faces. Practices that treat this as background noise aren't just losing visibility. They're baking legal exposure directly into their content calendar.
When practices ask why their articles stopped reaching patients, the answer is almost always the same. The content lacks clinical sourcing and structural integrity. Volume was never the lever. Verifiability was. It always has been.
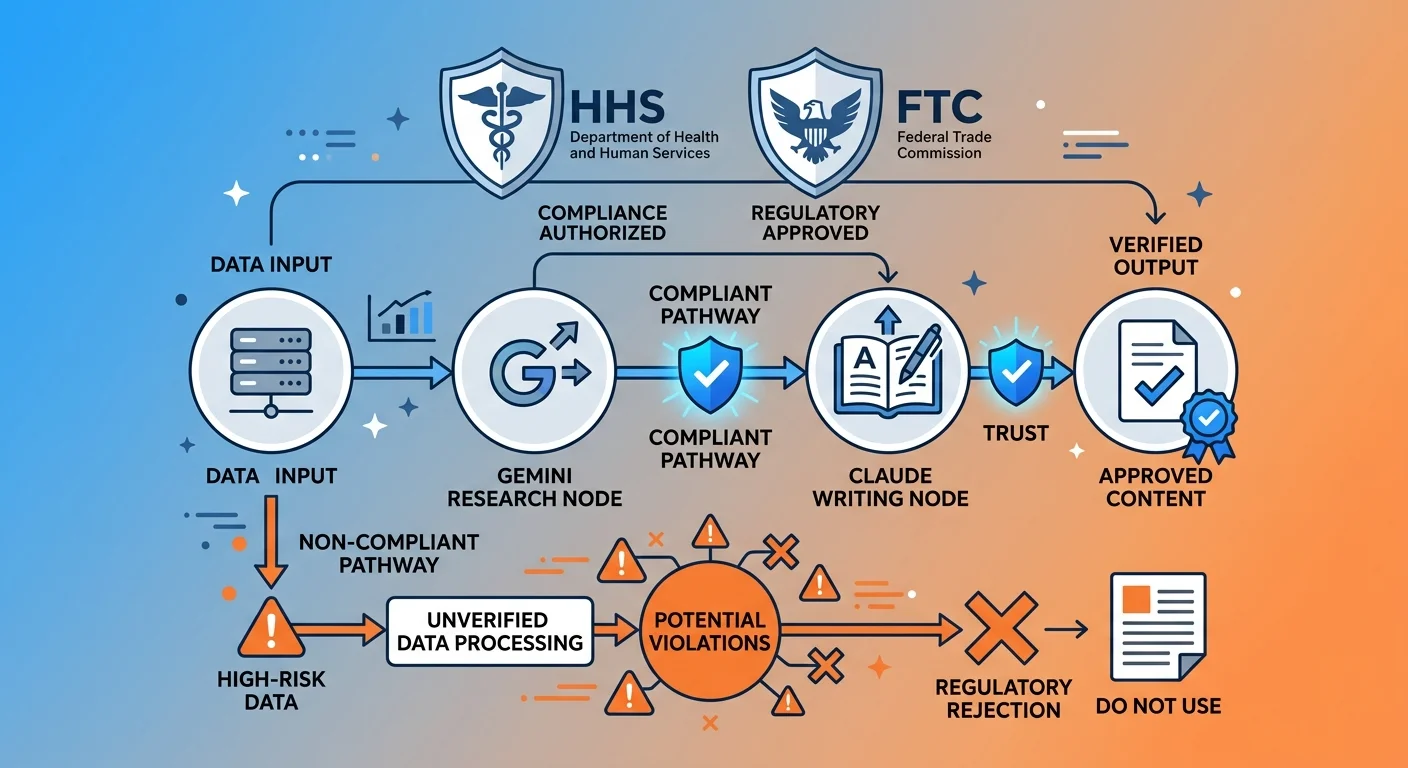
The Dual-AI Validation Difference
The dual-AI validation system — Gemini research into Claude writing, Gemini validation closing the loop — wasn't built because it sounded impressive. It was built because the regulatory and algorithmic reality of healthcare content made anything less indefensible.
Every claim in every article goes through a two-engine verification pass before it publishes. Sources are checked. Figures are traced to their origin. Clinical assertions are grounded in institutional-grade evidence. The FTC's pre-existing proof standard isn't a burden inside that model. It's the baseline the process is built around from day one.
That rigor is what separates iTech Valet AEO from any high-volume content operation. We don't publish vibes. We publish receipts. In the medical space, that distinction is the entire difference between a practice AI engines trust and one they quietly exclude from the answer.
| Regulatory Body | Requirement for AI-Assisted Content | Risk of Non-Compliance | How AI Authority Content Addresses It |
|---|---|---|---|
| FTC (Federal Trade Commission) | Companies must possess pre-existing scientific proof to support any AI-related healthcare marketing claims before content is published | Regulatory liability for any AI-assisted marketing claim that lacks verified, pre-existing scientific backing | Every claim is sourced and verified through a dual-AI validation pass before publication — the scientific evidence exists before the article goes live |
| HHS / ONC | HTI-1 rule mandates strict transparency metrics for predictive AI algorithms used in clinical decision support | Non-transparent AI-assisted clinical content fails to meet algorithmic accountability standards, creating compliance exposure | AI authority content is built on institutional-grade sources with traceable, schema-supported claims that satisfy transparency requirements |
Patient Trust, AI Recommendations, and the Visibility Gap
Here's the number that should stop you cold: 60% of U.S. adults say they'd feel uncomfortable if their own doctor relied on AI for their clinical care.
That's not a fringe group. That's the majority of your patient population — before they've booked a single appointment.
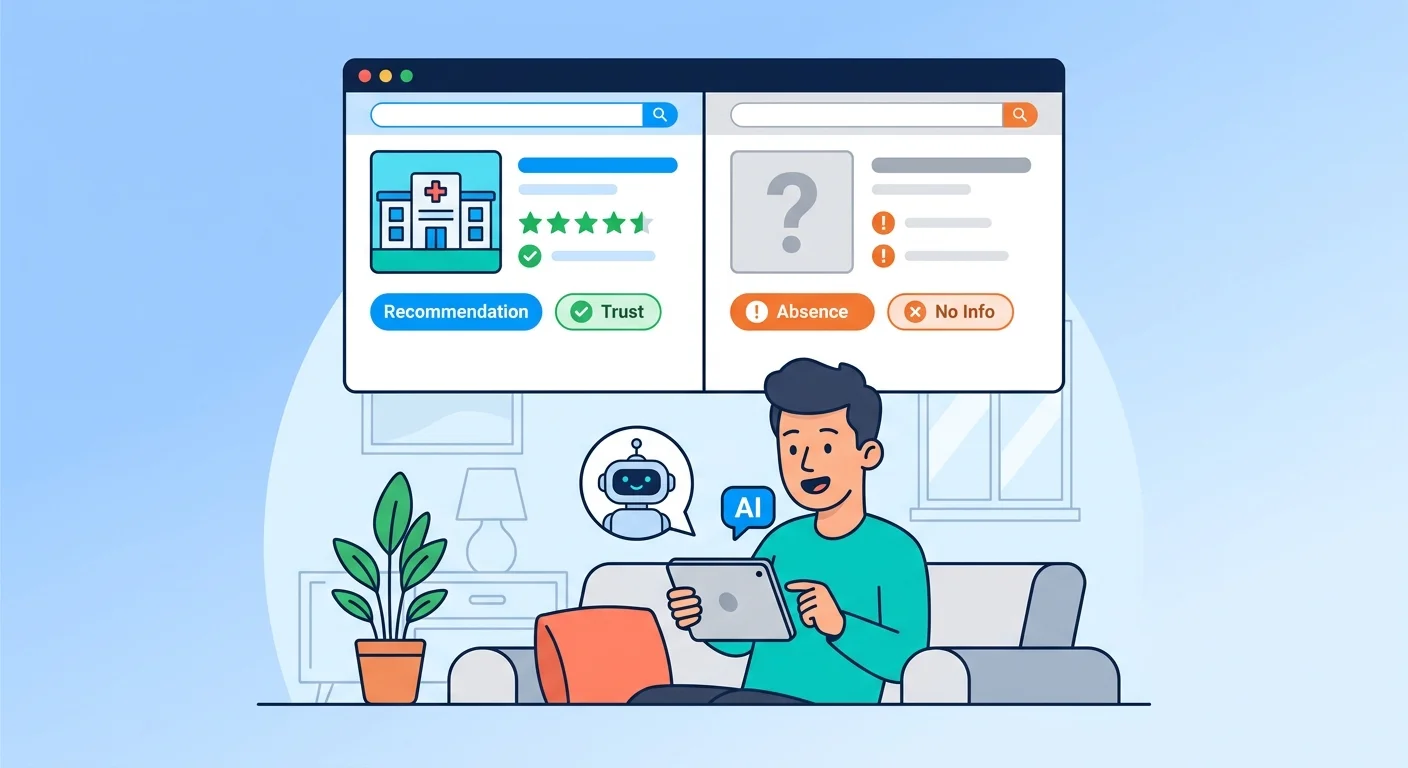
And yet those same patients are already asking AI engines who to see. They're typing their condition into ChatGPT. They're asking Gemini which clinic handles their specific issue. They're getting one name back — and booking based on it.
The discomfort with AI in the exam room doesn't stop anyone from using AI to choose which exam room to walk into. That contradiction is the entire problem.
So the practice AI names needs to feel credible before the patient ever walks in. That's the actual gap. Patients distrust AI in the exam room — which means the content AI is pointing them toward has to carry real clinical weight.
Generic, volume-produced content signals the opposite. It tells patients — and answer engines — that a practice treats its online presence the same way a content mill treats its output: interchangeable, unverified, disposable. The World Health Organization's governance guidelines exist precisely because unverified AI-generated medical content causes real-world harm. Patients sense that risk even when they can't name it.
What Patient Skepticism of AI Means for Your Content Strategy
Patient skepticism of AI isn't a problem to overcome. It's a signal to respect.
When 60% of U.S. adults express discomfort with AI-assisted clinical decisions, they're telling you exactly what your content has to prove: that a real, credible, clinically grounded practitioner is behind the practice — before the first appointment is ever booked.
And that's what Entity Trust actually delivers. Not rankings. Not traffic. A verified, structured, institutionally sourced body of content that signals to AI engines and the patients they refer: this practice knows its subject at a depth worth trusting.
The World Health Organization's framework for AI in healthcare puts hallucination safeguards and ethical content standards front and center — because the stakes in medicine are different from every other industry. Your content strategy has to reflect that. If it doesn't, AI engines will route patients to a practice whose content already does.
Volume-based content fails this test completely.
A hundred generic articles that any clinic in your market could have published don't tell AI engines — or patients — anything specific about yours. But verified, clinically sourced, schema-supported content does. It builds the semantic fingerprint that makes your name the one AI surfaces when a skeptical patient asks who they should trust.
The AI Visibility Check: Seeing the Gap in Real Time
Most practices assume they have reasonable AI visibility.
Most are wrong. The gap between where a practice thinks it stands and where AI engines actually place it is almost always larger than expected — and it stays invisible until someone runs the check.
The AI Visibility Check is a 15-minute diagnostic that shows exactly what ChatGPT, Gemini, and Grok say when a patient asks who to trust in your market.
Not an estimate. Not a proxy metric. The actual AI output — the name those engines surface when your ideal patient asks the question you need to own.
That data point changes everything. A practice that has seen the gap — in real time, from the same engines their patients use — understands exactly what Entity Trust is worth.
A practice that hasn't run the check is making content and infrastructure decisions without knowing what the actual problem is. In a space where patient trust is already fragile and the World Health Organization's governance standards are shaping how answer engines evaluate medical content, that's not a neutral position. It's a compounding liability. AI says your name or it doesn't — and guessing which one is true is a bet no medical practice can afford to keep making.
| Practice Content Profile | AI Recommendation Likelihood | Patient Trust Signal | Authority Gap Status |
|---|---|---|---|
| High-volume, generic articles with no clinical sourcing | Low — AI engines detect thin entity signals and route to more authoritative sources | Weak — patients sense interchangeable content and question clinical depth | Widening — competitors with structured authority content compound ahead |
| Keyword-optimized content without schema or structured data | Minimal — AI engines cannot parse or validate unstructured clinical claims | Unclear — content looks modern but lacks the institutional grounding patients trust | Stagnant — volume increases without closing the authority gap |
| Verified, institutionally sourced AEO content with schema integrity | High — AI engines recognize structured entity signals and cite the practice by name | Strong — patients encounter content that reflects real clinical depth before booking | Closing — every published article compounds the practice's semantic fingerprint |
| Dual-AI validated content with traceable clinical citations | Highest — satisfies both algorithmic trust thresholds and regulatory sourcing standards | Credible — content signals a practice whose claims can withstand scrutiny | Dominant — practice becomes the named recommendation AI engines default to |
| No active content strategy — static or outdated digital presence | None — AI engines have insufficient signals to associate the practice with any query | Absent — patients find no evidence of clinical expertise before the appointment | Critical — every month of inaction transfers authority to competitors who are publishing |
Frequently Asked Questions
Every question below came from a real practice owner who wasn't sold yet. Good. Skepticism is the right starting point.
Here's what they're all really asking: is this actually different from what we've already tried and paid for? It is. And the mechanism is the whole point.
Why does traditional healthcare SEO fail to rank your clinical voice in AI searches?
Traditional healthcare SEO was built to put pages in a ranked list. Keyword density, backlink volume, click-through rate — those were the levers. None of them matter when a patient asks ChatGPT a question and gets one name back.
AI engines don't scan lists. They evaluate entity credibility — schema integrity, institutional sourcing, semantic coherence, verified clinical grounding. Keyword articles don't build any of those signals. They never did.
Peer-reviewed research through the National Institutes of Health confirms that AI engines produce incomplete medical information when verified knowledge structures aren't in place. Content without clinical sourcing doesn't just fail to get cited. It registers as the kind of noise AI engines are designed to filter before they ever form a response.
Is AI Authority content safe from HIPAA and regulatory healthcare penalties?
Safe when built correctly. That phrase does a lot of work — so let's be precise about what 'correctly' means.
The FTC's position isn't subtle: companies making AI-related claims in healthcare marketing must have pre-existing scientific proof behind those claims. Not eventually. Before anything publishes. That's the compliance floor right now.
The dual-AI validation process — Gemini research into Claude writing, validated by Gemini and refined by Claude — is built around that standard from the start. Every claim is sourced before it publishes. Every figure traces to an institutional origin. Content built that way isn't a liability. It's a defensible asset.
Volume-produced content without clinical sourcing is the liability. Every unsourced assertion sitting under a practice's name is an exposure point. The FTC has already signaled it will pursue exactly that.
How does iTech Valet build Entity Trust for medical practices compared to standard SEO?
Standard SEO chases keyword positions. Entity Trust is built through a completely different mechanism — and conflating the two is why most practices end up invisible.
SEO agencies optimize page structure for a search algorithm. The Local AI Authority Engine constructs the verified signals AI engines use to confirm a practice's identity. Schema markup that tells AI engines exactly who the practice is. Institutionally sourced clinical content that anchors authority to verifiable external knowledge. Semantic coherence built across every article so the practice's name accretes meaning over time.
That compounding semantic fingerprint is what forces an AI engine to name a specific practice instead of a competitor.
SEO builds a ranked position. Entity Trust builds a recommendation. In healthcare — where 60% of U.S. adults already feel uncomfortable with AI in clinical settings — the depth and verifiability of that trust signal is the difference between a name patients act on and one they scroll past. ITech Valet engineers the signal. SEO agencies optimize the page. Those aren't variations of the same job.
What are the clinical risks of using high-volume commodity content mills?
The risks run in both directions. Neither is good.
First: high-volume commodity content generates medical assertions without institutional sourcing. That puts a practice's name on claims it can't defend if a patient, regulator, or competitor challenges them. The FTC is unambiguous — AI-assisted healthcare marketing requires pre-existing scientific evidence. Content mills aren't built to produce that.
Second: the structural omission risk is documented. Peer-reviewed research through the National Institutes of Health finds that AI tools disseminate incomplete medical content and miss nuanced patient directives when operating without verified knowledge frameworks. A practice outsourcing content to a volume operation is delegating clinical communication to a process with no mechanism for clinical accuracy.
What you're left with is a digital footprint that looks active and functions as a liability. Busy is not the same as trustworthy. In healthcare, AI engines and regulators both know the difference.
How long does a clinic take to build enough Citation Velocity to dominate ChatGPT and Gemini?
Any agency that gives you a specific number of months is selling you a timeline, not a result. There's no honest answer that works that way.
What is clear: the clock doesn't start when you publish articles. It starts when you publish the right kind — verified, structured, institutionally sourced, schema-supported. Citation Velocity builds as AI engines encounter consistent, credible signals from a practice's entity over time.
Practices that compound fastest are the ones that build the right foundation first and execute consistently against it. Practices that chased volume first have to unwind bad signals before the right ones can accumulate. That adds time — it doesn't remove it.
Start right. Execute consistently. The velocity follows. That's not a promise. It's a description of the mechanism.
What is the difference between Semantic Density and keyword density in healthcare content?
Keyword density tells a search algorithm how often a term appears on a page. Semantic Density tells an AI engine how deeply a practice understands a subject. Those aren't variations of the same measure.
Keyword density is a frequency metric. Semantic Density is a depth metric — built by covering a clinical topic from multiple angles, connecting it to verified institutional knowledge, and creating enough conceptual coverage that AI engines can map a practice's authority across a subject area, not just a phrase.
In healthcare, this distinction is decisive. Peer-reviewed findings through the National Institutes of Health confirm that AI engines disseminate incomplete medical information without verified knowledge structures in place. A practice building Semantic Density — real clinical depth, sourced and structured — becomes the entity AI engines trust to give patients accurate answers.
A practice optimizing for keyword density is solving for a mechanism AI search has already moved past. The engine isn't counting words anymore. It's evaluating understanding.
The Verdict on Volume
Volume never built AI authority. In healthcare, it actively destroys it.
AI engines don't reward publishing frequency. They reward clinical depth, verified sourcing, and the structural signals that tell an answer engine a practice is worth citing. Generic content at scale produces exactly one thing: a digital footprint that looks busy and means nothing to the engines your patients are already using.
Every element of AI authority content exists to answer one question AI engines ask about every practice: is this the name worth saying?
The dual-AI validation. The institutional sourcing. The schema integrity. The semantic fingerprint built article by article over time. None of that is decoration. It's a direct answer to the trust evaluation answer engines run before they ever form a response.
High-volume content mills can't answer that question. They aren't built to. They're built to produce output — not authority. And in a space where patient trust is already fragile and regulatory standards are tightening from every direction, the gap between output and authority is the gap between being recommended and being invisible.
Here's the hill iTech Valet will die on: AI visibility in the medical space is an infrastructure problem. Not a publishing problem.
The practices that own AI recommendations six months from now are building verified Entity Trust today. Not flooding the web with interchangeable articles and hoping an algorithm notices. The ones that wait are ceding ground that compounds in someone else's favor — every single month, without pause.
That's not a prediction. That's the mechanism. And it's already running.
AI says your name or it doesn't. The only question left is what you're doing about it.
AI is already answering that question in your market. Either your name is the answer — or a competitor's is. Run the AI Visibility Check and find out which one.
621 Enterprises, Inc. | Copyright 2026 | All rights reserved