
Is AI Authority Content Safe for Healthcare? A Look at Compliance and Risk
AI Authority content is safe for healthcare — but only when every claim traces back to a verifiable source. Raw, unmoderated AI output doesn't meet that bar. It's a liability.
The risks aren't theoretical. The World Health Organization warned that rapid adoption of untested large multimodal models leads to healthcare provider errors and direct patient harm. The Federal Trade Commission put healthcare businesses on notice: unsupported AI-generated health claims require scientific proof, and operating without it makes you an enforcement target. The FDA has authorized over 950 AI and machine-learning-enabled medical devices — but unauthorized diagnostic claims in marketing content are still a federal violation, regardless of that number. HIPAA rules enforced by the Department of Health and Human Services require executed Business Associate Agreements before any healthcare software can legally process Protected Health Information.
The public trust picture is just as stark. Pew Research Center found that 60% of U.S. adults feel uncomfortable with healthcare providers relying on AI for diagnosis or treatment recommendations. Publishing unverified AI content doesn't close that gap. It widens it.
Peer-reviewed clinical evaluations confirm what regulators are already acting on: large language models frequently hallucinate citations and produce medically inaccurate information that fails clinical review. Unmoderated AI output in a healthcare context isn't just a reputational problem. It's a patient safety problem.
The answer isn't to avoid AI content. It's to engineer it correctly. An AI Authority content strategy built on multi-layered factual verification — where every claim is sourced, every citation is real, and every output is validated before publication — turns AI content from a compliance threat into a compounding authority asset. Regulators want receipts. AI engines trust receipts. Patients respond to receipts.
Last Updated: July 10, 2026
- • Why Raw AI Output Is a Liability Trap for Healthcare Practices
- • The Regulatory Bodies Already Watching Healthcare AI Content
- • What Compliant AI Authority Content Actually Requires
- • Who Should — and Shouldn't — Be Running AI Authority Content in Healthcare
-
• Frequently Asked Questions
- • Is raw ChatGPT output safe to publish on a medical or chiropractic website?
- • How do regulatory bodies like the FTC view healthcare claims generated by AI?
- • What is the liability risk for a clinic using unverified AI-written medical content?
- • Does AI-generated medical content violate search engine or AI engine spam guidelines?
- • How does a Two-AI Validation System prevent clinical misinformation in healthcare content?
- • Does HIPAA apply to AI tools used in healthcare content creation?
- • The Bottom Line on AI Authority Content and Healthcare Compliance
Why Raw AI Output Is a Liability Trap for Healthcare Practices
Raw AI output doesn't know what it doesn't know. It generates confident, clinical-sounding prose that fails peer review — and the practice that publishes it owns every word of that liability. The model doesn't.
That's not speculation. Published clinical analysis confirms that large language models frequently hallucinate citations and generate medically inaccurate information that doesn't survive clinical scrutiny. The error doesn't live in the AI. It lives in the content that gets published without a verification layer sitting between the model's output and your audience.
And the patients reading that content aren't giving anyone the benefit of the doubt. 60% of U.S. adults already feel uncomfortable when their healthcare provider relies on AI for diagnosis or treatment. Publishing unverified AI-generated health claims doesn't ease that discomfort. It weaponizes it. Every piece of content a practice puts out either builds trust or burns it — and raw AI output, by default, burns it.
Why Unverified AI Content Fails on Two Fronts
Here's the thing — it fails in two directions at once. Regulatory. Clinical. And those two failures don't stay in their lanes.
The FTC doesn't distinguish between intentional deception and negligent AI output. If you publish an unsupported health claim, you're the one with the enforcement problem — full stop. That's exactly why practices serious about compliance are making the shift to AI Authority content as a regulatory imperative, not a marketing upgrade. Content that can't show its work isn't safe to publish. Period.
A hallucinated citation looks identical to a real one in a published article. A patient acts on it. A regulator finds it. Neither the AI model nor the content platform absorbs that outcome — the practice does. The only escape from that exposure is a verification architecture that catches the hallucination before it publishes. Not after. An AEO Content Strategy built on source-backed, receipt-generating validation is what separates compliant authority content from a liability waiting to surface.
| Risk Category | What It Looks Like in Practice | Potential Consequence |
|---|---|---|
| Clinical Misinformation | AI generates confident, clinical-sounding content containing hallucinated citations or inaccurate treatment information that reads as authoritative | Patients act on false health guidance; practice absorbs the liability when a regulator or injured party traces the content back to publication |
| FTC Enforcement Exposure | Unsupported health efficacy claims appear in published AI-generated content without scientific backing or source attribution | Federal Trade Commission treats negligent AI output the same as intentional deception — the publishing practice is the enforcement target |
| FDA Marketing Violations | AI-written content makes diagnostic or treatment claims that exceed the scope of any cleared medical device or software authorization | Publishing unauthorized diagnostic claims in marketing content constitutes a federal violation regardless of a practice's overall compliance record |
| HIPAA Data Risk | AI tools process or are trained on patient intake information, symptom descriptions, or case details without an executed Business Associate Agreement | HHS treats any unauthorized transmission of Protected Health Information as a reportable breach — exposure scales with the volume of data involved |
| Eroded Patient Trust | A practice publishes AI-generated health content with no visible verification layer, source attribution, or clinician review signal | Patients who already distrust AI in clinical settings disengage — content that can't show its work actively undermines the authority it was meant to build |
| AI Engine Rejection | Raw, unsourced AI output lacks the entity trust signals, structured citations, and verified authority markers that AI recommendation engines require | Content gets ignored or deprioritized by AI engines in favor of source-backed, receipt-generating authority content from competitors who built the infrastructure correctly |
The Regulatory Bodies Already Watching Healthcare AI Content
Three federal agencies are already watching: the FTC, FDA, and HHS. Each owns a different slice of the AI content compliance picture. And none of them are coordinating with each other to give your practice a pass.
That's the part most practices get wrong.
They assume compliance means one policy, one agency, one inbox. It's three overlapping enforcement frameworks — each with distinct triggers. AI-generated content can trip all three at once. The practice never sees it coming until someone's already asking questions.
Every regulator is asking the same core question from a different angle: can you show your work?
Content that can't answer that is exposed to all three agencies simultaneously. Content built on how AI authority amplifies clinical trust — sourced claims, verified citations, a documented validation layer — can answer it. That's not a marketing edge. That's the minimum bar for compliance.
FTC, FDA, and HHS: Three Agencies With Three Different Problems
The FTC's reach is the widest. Their March 2023 guidance doesn't include a 'we didn't mean to' exemption.
Publish an AI-generated claim about what your services do for a patient's health — and back it with nothing — and the FTC treats it as a deceptive health claim. Full stop. The AI model doesn't take the enforcement call. The practice does.
FDA guidance makes the boundary clear: over 950 AI and machine-learning-enabled medical devices have been authorized. That authorization doesn't touch marketing content making unauthorized diagnostic claims.
Pointing to cleared AI software doesn't make your content compliant. Device clearance and content compliance are two entirely separate tracks. Conflating them is exactly the assumption that creates federal exposure.
HHS lands the third hit through HIPAA. Published health app compliance rules are direct: any healthcare software processing Protected Health Information must have executed Business Associate Agreements before that data transmission is legal.
If an AI content tool ingests patient context — even indirectly, even in a draft-suggestions workflow — and there's no BAA in place, the practice isn't just publishing risky content. It's already in a HIPAA violation. At that point, the content is the smallest problem on the table.
| Regulatory Body | Primary Jurisdiction | Key Healthcare AI Content Rule | Enforcement Risk |
|---|---|---|---|
| Federal Trade Commission (FTC) | Marketing claims and consumer protection across all industries, including healthcare | AI-generated health claims must be backed by scientific proof — publishing unsupported claims about what a service or treatment can do is treated as deceptive advertising regardless of whether a human or an AI wrote it | Enforcement action, civil penalties, and mandatory corrective advertising — the practice absorbs full liability for content published under its name |
| Food and Drug Administration (FDA) | Medical devices and software, including AI/ML-enabled diagnostic and treatment tools | Device clearance and content compliance are two separate tracks — having cleared AI software does not authorize a practice to make diagnostic or treatment claims in published marketing content | Federal violation for unauthorized diagnostic claims in content; no safe harbor from device authorization status |
| Department of Health and Human Services (HHS) — HIPAA | Protected Health Information (PHI) in digital health environments, including software and apps used in patient care workflows | Any healthcare software processing PHI requires executed Business Associate Agreements before data transmission is legal — this applies to AI content tools that touch patient context, even indirectly | HIPAA breach exposure, HHS investigation, and civil monetary penalties — content liability becomes secondary to the underlying data compliance failure |
| World Health Organization (WHO) | International guidance on safe adoption of large multimodal models in clinical settings | Rapid deployment of untested AI systems in healthcare contexts risks provider errors and direct patient harm — WHO guidance calls for rigorous evaluation before clinical or health-adjacent use | Reputational and institutional risk; non-binding at the federal level but cited by domestic regulators as the international safety standard |
What Compliant AI Authority Content Actually Requires
Knowing the rules is the easy part. Building a workflow that survives them is where most practices have nothing.
Compliant AI Authority content isn't what you get when a human skims AI output before hitting publish. It's a production process with a documented chain of custody. Every claim traces to a verifiable source. Every citation gets confirmed against the original. The validation layer is on the record before anything goes live.
The WHO's January 2024 guidance named hallucination and biased training data as core risks of rapid LMM adoption. Those risks don't disappear because someone read through the draft. They disappear when verification is systematic — built into the process, not bolted on as an afterthought.
That's the line between volume and depth. A content approach that demands depth over raw output forces every claim to earn its place — sourced, confirmed, traceable.
It's not slower. It's the only kind AI engines and federal regulators actually trust.
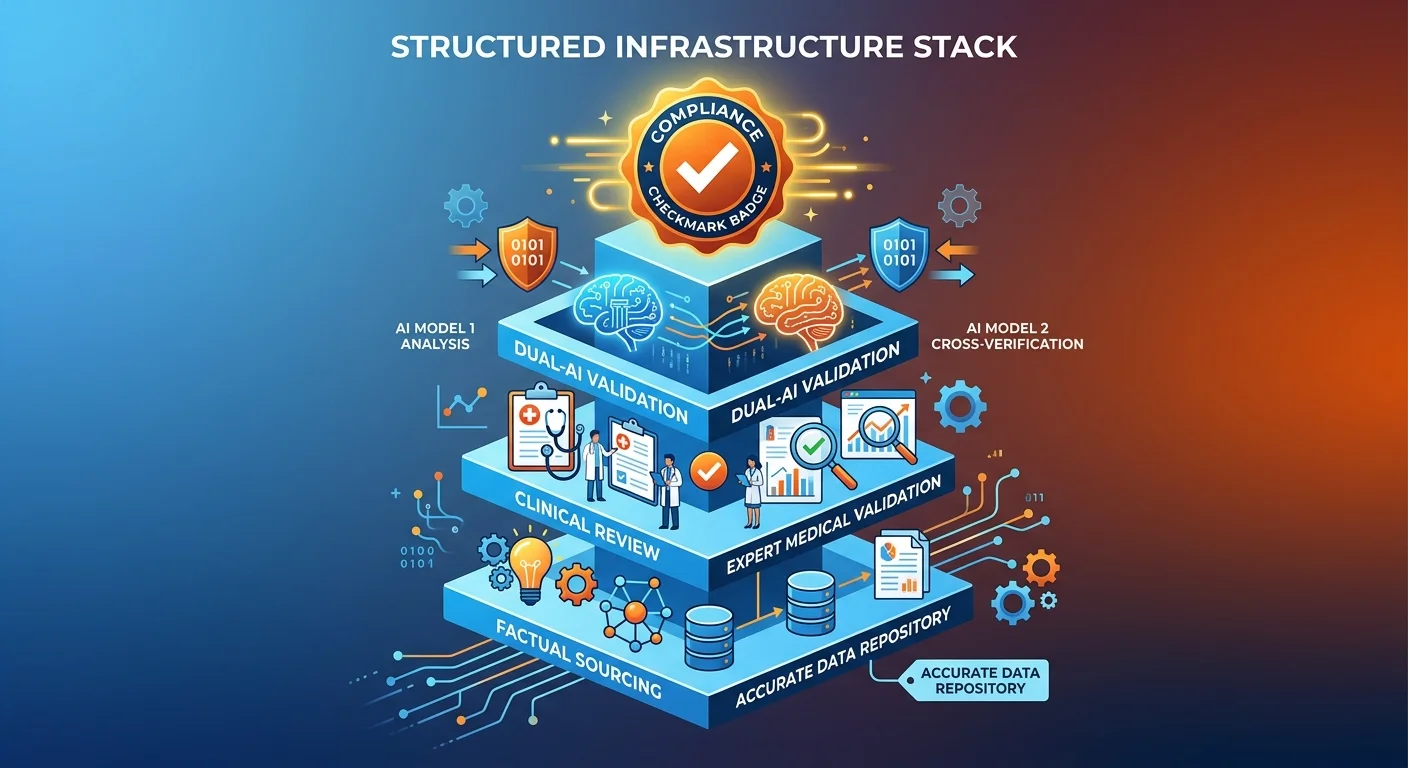
The Verification Stack: What Safe Execution Looks Like
A verification stack isn't one thing. It's a sequence. Collapse any part of it, and you've created the exact exposure you were trying to avoid.
The first layer is source grounding. Every factual claim in an AI Authority article must trace to a real institutional source — a peer-reviewed publication, a federal agency, an industry research body. Not a general AI summary. Not a content farm rewrite.
Here's why that matters: clinical hallucinations pass undetected because the prose sounds authoritative. The only counter is a citation check that goes source-to-source. Prose-to-prose comparison catches nothing.
HIPAA compliance is the second mandatory layer. If any tool in the workflow touches Protected Health Information, a Business Associate Agreement must be in place before a single word of content is produced. That's an HHS requirement — not a best practice someone can deprioritize.
The final layer is pre-publication validation. Not a read-through. A structured review that confirms every claim survives scrutiny by the standards of the agencies watching.
That's what the AEO Content Writing Services framework is built to deliver — a receipt-generating production process where every output can show its work to the FTC, the FDA, and HHS at the same time.
Practices that build this stack don't just avoid liability. They build verified authority infrastructure that AI engines recognize as trustworthy — and recommend.
| Compliance Requirement | Why It Matters for Healthcare | What Failure Looks Like |
|---|---|---|
| Source-Grounded Factual Claims | Every clinical assertion a practice publishes creates a liability record. If a claim can't be traced to a verifiable institutional source, the practice — not the AI model — owns the enforcement exposure when a regulator or patient disputes it. | AI-generated prose that sounds authoritative gets published without a citation check. A patient acts on a hallucinated treatment claim. The practice has no documentation trail showing the claim was verified before it went live. |
| Licensed Clinician Review Layer | Peer-reviewed clinical standards require that health information be evaluated by someone with the credentials to catch medically inaccurate content. AI output alone cannot satisfy that standard — the review layer is what converts raw output into defensible content. | A human skims AI-generated health content without clinical expertise and approves it. The article contains a subtly inaccurate treatment recommendation. Neither the skimmer nor the AI flagged it — and it publishes. |
| HIPAA-Compliant Tool Workflow | Any software in the content production process that touches Protected Health Information requires a signed Business Associate Agreement before use. This is an HHS compliance requirement — not a recommendation — and it applies to AI tools regardless of how peripheral their role appears. | An AI drafting tool ingests patient context or clinical notes as part of a 'personalization' workflow. No BAA exists. The content liability is secondary — the practice is already in a HIPAA violation before a word is published. |
| FTC-Safe Claim Standards | The FTC treats unsupported health efficacy claims as deceptive advertising regardless of whether the content was AI-generated or human-written. Every claim about what a clinical service can do for a patient's health must be backed by scientific proof — or it creates federal enforcement risk. | An AI content tool generates confident benefit language about a chiropractic adjustment technique. No scientific backing is cited. The practice publishes it. The FTC doesn't ask whether the practice knew the claim was unsupported — it asks whether the claim was. |
| Documented Validation Before Publication | A verification layer that runs before publication — not after — is the only structure that prevents regulatory exposure from compounding. Documentation of that process is what allows a practice to 'show its work' to any agency that asks. | A practice runs a post-publication review after a complaint surfaces. By that point the content is indexed, cited, and potentially acted upon. The validation happened too late to matter — and the absence of pre-publication documentation makes the defense weaker, not stronger. |
| AI Engine Trust Signals | AI answer engines apply their own credibility filters when deciding whose content to surface. Content built on verifiable sources, traceable citations, and structured authority infrastructure earns entity trust. Content that can't show its work doesn't get recommended — it gets ignored. | A practice publishes high-volume AI content with no source grounding and no structural authority signals. The content looks prolific but reads as generic to AI engines. Competitors with lower output volume but higher verified authority get cited instead. |
Who Should — and Shouldn't — Be Running AI Authority Content in Healthcare
Here's the thing: this isn't for everyone. And saying that out loud is part of what makes an AI Authority strategy credible.
The practices that get results from a verified content stack share one defining trait: they want accuracy over volume. They understand that what makes an AI Authority article trustworthy isn't publish speed — it's the verification layer underneath every claim. And they're willing to run a production workflow that can show its receipts to the FTC, the FDA, and HHS on demand.
Here's the number that makes this concrete. Pew Research Center found that 60% of U.S. adults are already uncomfortable with AI in their clinical care. That discomfort doesn't disappear when a practice publishes AI-generated content. It either gets defused by source-backed authority — or it compounds into distrust. The FTC, the FDA, and HHS aren't waiting for patients to complain before they move. Practices ready for AI Authority content understand that dynamic. The ones that don't aren't ready.
The Practices That Get Results — and the Ones That Don't
The practices that get results aren't chasing volume. They're building verified authority — one sourced, receipt-generating article at a time. Every published claim is a commitment they're prepared to defend. Not a marketing line written for clicks.
The Local AI Authority Engine is built for that practice. Not for the ones hunting a shortcut. For the ones that want the AI recommendation — and know that earning it requires infrastructure, not just output.
The practices that don't get results are easy to spot. They want high-volume output with minimal oversight. BAA compliance isn't on their radar. Source verification slows them down. They want content fast. The World Health Organization named exactly this pattern in its January 2024 guidance as the core risk vector — rapid AI adoption without the verification architecture to catch hallucinations before they publish. That's not an AI Authority strategy. That's a liability pipeline.
| Practice Profile | AI Authority Content Fit | Primary Risk if Misapplied |
|---|---|---|
| Accuracy-first practice with clinician oversight on all published content | Strong fit — verification layer is already part of the clinical culture | Minimal — the practice is structurally prepared to catch errors before they publish |
| Established practice building long-term authority in a defined geographic market | Strong fit — compounding authority asset aligns with a multi-year growth model | Low if the workflow includes source grounding and BAA compliance from day one |
| Practice with a clear specialty or clinical niche and documented patient outcomes | Strong fit — depth-first content maps directly to the specificity AI engines reward | Low — narrow scope reduces hallucination surface and strengthens citation accuracy |
| Volume-first practice seeking fast content output with minimal human review | Poor fit — speed requirements conflict with the verification layer the strategy requires | High — unverified claims published at scale create compounding regulatory exposure across FTC, FDA, and HHS simultaneously |
| Practice unwilling to execute Business Associate Agreements for AI tools in the content workflow | Disqualifying — BAA compliance is a hard legal prerequisite, not a preference | Severe — any AI tool processing patient-adjacent data without a BAA is already inside a HIPAA violation before the first article publishes |
| Generalist practice with no defined clinical voice or patient authority positioning | Weak fit — AI Authority content requires a clear entity signal that AI engines can recognize and cite | Moderate — generic, undifferentiated content fails to build entity trust and produces no compounding authority value |
Frequently Asked Questions
Here's where it gets real. These are the questions practices actually ask — the ones where a wrong answer creates downstream exposure that doesn't go away.
Not hypotheticals. These are the friction points that stall real decisions — and silence on any of them is its own expensive answer.
Is raw ChatGPT output safe to publish on a medical or chiropractic website?
No. Raw LLM output isn't publication-ready for any healthcare practice — and the problem isn't the writing. It's the sourcing.
Large language models hallucinate. They generate medically inaccurate citations and clinical claims that don't survive scrutiny. The prose sounds credible. The underlying sourcing frequently isn't.
Publish that output without a verification layer and the practice owns every unverified claim in front of the FTC, the FDA, and HHS. None of them accept "the AI wrote it" as a defense. Not one.
How do regulatory bodies like the FTC view healthcare claims generated by AI?
The FTC doesn't draw a line between human-written and AI-generated health claims. Their March 2023 guidance is explicit: any health efficacy claim requires scientific proof before it publishes.
If an AI tool drafts a statement about what a chiropractic adjustment does for a patient's condition — and that statement isn't backed by verifiable evidence — the FTC treats it as a deceptive health claim.
The practice faces the enforcement action. The AI model doesn't. That's not a technicality. That's the rule.
What is the liability risk for a clinic using unverified AI-written medical content?
The exposure doesn't come from one agency. It comes from three — at the same time.
The FTC goes after deceptive health claims without verified scientific backing. The FDA draws a hard line between cleared AI software and what you're allowed to say in published marketing copy — device authorization doesn't cover unverified diagnostic statements. And HHS enforces HIPAA compliance for any AI tool that touches Protected Health Information without an executed Business Associate Agreement.
That's not one risk. That's three separate enforcement bodies, running three separate exposure tracks, none of them coordinating to give anyone a break.
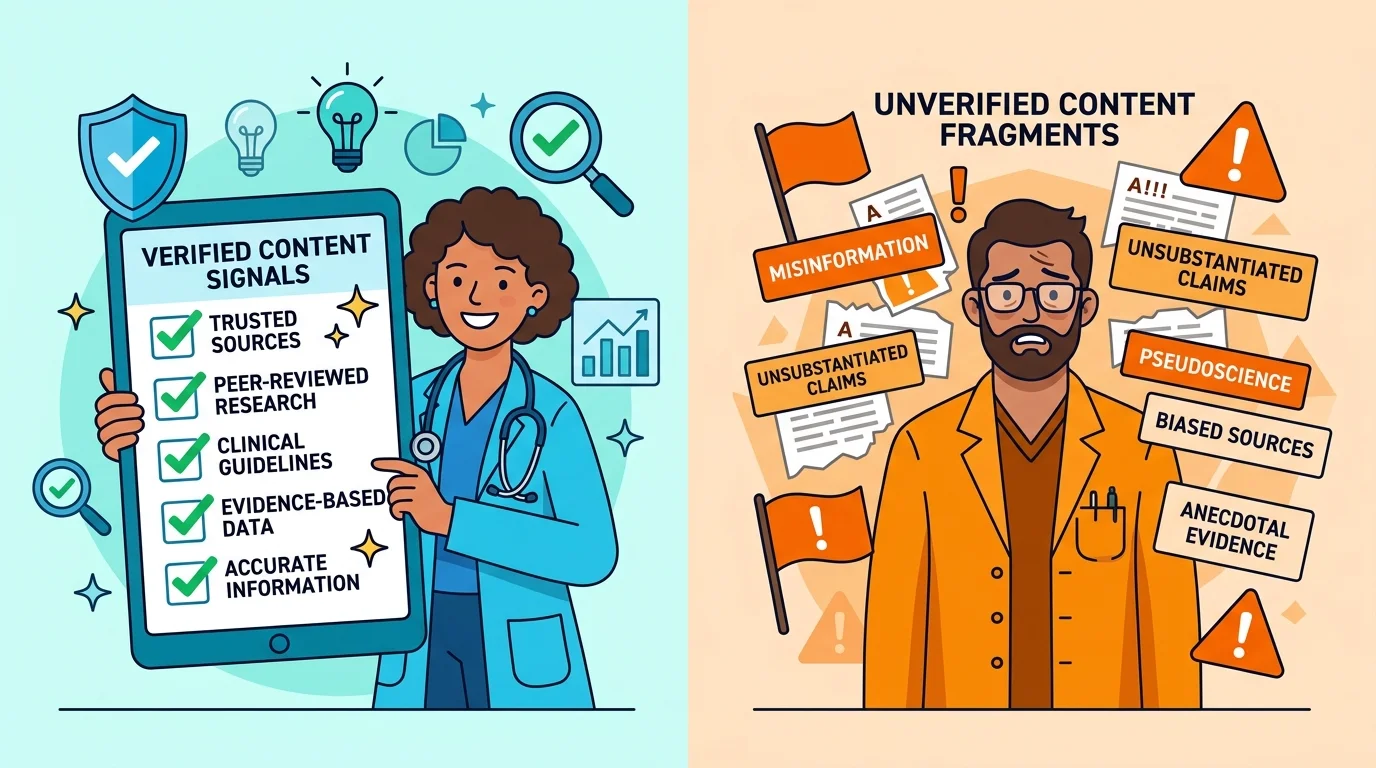
Does AI-generated medical content violate search engine or AI engine spam guidelines?
AI engines are trained to deprioritize content that reads as low-quality, unverified, or mass-produced. Healthcare content gets extra scrutiny — because recommending clinical misinformation carries a higher cost than getting a restaurant recommendation wrong.
So here's what actually happens: a clinic publishing raw, unchecked AI output isn't just creating regulatory exposure. It's producing content the AI engines it needs to trust it are actively built to avoid recommending.
Unverified output loses on both fronts. Compliance and authority. At the same time. That's not a tradeoff — that's just failure on two tracks instead of one.
How does a Two-AI Validation System prevent clinical misinformation in healthcare content?
A Two-AI Validation System removes the single-pass assumption from the production process entirely. One AI generates. A second AI validates — cross-checking every claim against its cited source, flagging hallucinations, and confirming what the content says actually matches what the institutional source published.
Clinical hallucinations slip through when the check is prose-to-prose. They don't slip through when the check is source-to-source.
That's the structural difference. And it's the only verification architecture that produces a real receipt — the kind that holds up when a regulator or an AI engine looks at it.
Does HIPAA apply to AI tools used in healthcare content creation?
Yes — and the rule is stricter than most practices expect.
HHS is unambiguous: any healthcare software that processes Protected Health Information requires an executed Business Associate Agreement before that data transmission is legal. And "processing" isn't limited to storing patient records. If an AI content tool ingests any patient-adjacent context — even inside a drafting workflow — with no BAA in place, the practice is already in a HIPAA violation. Before a single word publishes.
The content risk is secondary. The data compliance failure is the primary exposure. And it starts the moment the tool is used — not the moment the article goes live.
The Bottom Line on AI Authority Content and Healthcare Compliance
Here's the bottom line.
AI Authority content in healthcare is safe when it's built on receipts. It's dangerous when it isn't.
That's not a nuance. That's the whole compliance picture in one sentence. The FTC demands scientific proof for health efficacy claims — no exceptions, no 'we didn't mean to' carve-out. The FDA draws a hard line between cleared AI software and what you're allowed to publish in your marketing — device authorization doesn't touch your content strategy. Every agency is asking the same question from a different angle: can you show your work? The practices that can answer yes are building authority. The ones that can't are building exposure.
The receipt metaphor isn't rhetorical. It's structural.
Every claim in a verified AI Authority article traces to an institutional source. Every citation is confirmed before it publishes. Every output can survive simultaneous scrutiny from every regulatory body already watching — without needing a pass from any of them.
That's what turns AI content from a liability pipeline into a compounding authority asset. Not the model. Not the volume. The verification architecture underneath it.
The practices that earn the AI recommendation aren't the ones publishing the most. They're the ones that can show their work — claim by claim, source by source, article by article.
That's what iTech Valet is built to deliver. Not content for its own sake. Verified authority infrastructure that AI engines trust and regulators can't challenge.
The gap between safe and dangerous AI content in healthcare comes down to one thing. Publish receipts, not vibes — or don't publish at all.
The compliance clock doesn't wait for you to feel ready. Run the AI Visibility Check and find out exactly where your practice stands — before a regulator, a search engine, or a patient does it for you.
621 Enterprises, Inc. | Copyright 2026 | All rights reserved