
How AI Authority Content Deepens Patient Trust Instead of Destroying It
AI authority content deepens patient trust when it's built on verified, structured information. It destroys trust when it isn't. The difference has nothing to do with whether AI was involved in creating the content. The difference is whether the content functions as a receipt or a vibe.
Receipts, not vibes. That's the whole game.
Over 74% of patients use search engines and medical platforms to research symptoms and evaluate local clinical credentials before booking an appointment. That research doesn't end at a list of blue links anymore. ChatGPT, Gemini, and Grok now construct structured citations to recommend medical entities based on verifiable web trust indices. When a patient asks one of those engines who the best chiropractor in their area is, the engine produces one answer. That answer is built from Entity Trust, Citation Velocity, and Semantic Density — not keyword density, not backlink counts.
The trust barrier is real. Approximately 60% of U.S. adults express discomfort with healthcare providers relying on artificial intelligence for their medical care. But that discomfort isn't aimed at authoritative, factually validated clinical content. It's aimed at generic, unverified output that reads like no human expert was ever involved. More than 80% of healthcare consumers say access to peer-reviewed, factually validated patient education directly impacts their choice of clinician.
That's the gap. Patients distrust AI content that lacks verification. They seek out — and trust — content that's structured, sourced, and authoritative.
Traditional search engine volume is projected to drop by 25% by 2026 as conversational AI agents replace the old list-based model. The practices waiting for that shift to become obvious are handing authority to competitors who moved first. AI authority content — built with verified sources, proper schema, and tight entity signals — isn't a threat to patient trust. It's the mechanism that earns it.
Last Updated: June 12, 2026
- • Why Generic AI Content Destroys Patient Trust (And What's Actually Going On)
- • What AI Engines Actually Look for When They Decide to Trust a Practice
- • How the AI Authority Engine Turns Clinical Content Into Patient Trust at Scale
- • What Verified AI Authority Content Looks Like Versus What Most Practices Publish
-
• Frequently Asked Questions About AI Authority Content and Patient Trust
- • How does AI authority content build patient trust rather than alienating them?
- • Why do generic AI blog posts fail to satisfy generative engine standards?
- • What makes patient-facing clinical content readable and authoritative to both humans and AI engines?
- • How do structural citations and schema play a role in deepening patient trust on AI platforms?
- • Can an AI Visibility Check reveal why patients are finding my local competitors instead of me?
- • The Receipt Is the Strategy
Why Generic AI Content Destroys Patient Trust (And What's Actually Going On)
Patients aren't afraid of AI. They're afraid of being lied to by something that sounds confident.
Generic AI content — the kind agencies run through the same prompt for fifty different clients — reads like nobody involved has ever treated a patient. No clinical grounding. No sourcing. No actual conviction behind any claim. Patients feel that instantly. And the moment they feel it, the trust is gone.
Over 74% of patients use search engines and medical platforms to research symptoms and evaluate local clinical credentials before booking an appointment. They're not browsing. They're auditing. When they land on thin, unverified output that reads like a vibe instead of a receipt, the practice loses the appointment before the phone ever rings.
Why Most AI-Generated Health Content Fails the Trust Test
The failure isn't that AI was used. It's that the content wasn't built to withstand scrutiny.
ChatGPT, Gemini, and Grok don't rank content by how smooth it reads. They cross-reference it against verifiable trust indices — Entity Trust, Citation Velocity, Semantic Density. Content without those signals doesn't get cited. It doesn't matter how clean the prose is. If the underlying structure doesn't check out, the engine won't say your name.
Approximately 60% of U.S. adults express discomfort with healthcare providers relying on artificial intelligence for their care. That's not a red light — it's a direction. The discomfort isn't with AI. It's with unverified, uncredentialed output dressed up as clinical authority. More than 80% of healthcare consumers say access to factually validated patient education directly shapes their choice of clinician. Structured, sourced content built around a real provider's real expertise reads differently. Patients feel it. So do the engines recommending providers to them.
The Agency Industry's Role in the Trust Problem
The agency industry created this problem. It's still selling the same broken fix. The standard retainer model — pay a monthly fee, get a batch of loosely relevant posts with no schema, no entity signals, no clinical sourcing — was already underperforming before conversational AI arrived. Now it's actively harmful.
Agencies optimized for volume. Twelve posts a month, loosely targeted, published on a schedule, reported as "content delivered." But what they weren't building — and still aren't — is the structured authority infrastructure that generative engines use to decide whose name to say. That gap is exactly why most practices are invisible right now. And it's exactly why shifting from agency retainers to an AI authority engine isn't a nice-to-have — it's the entire fix. most AI authority agencies fail chiropractors
Receipts, not vibes. Agencies sold impressions, click-through rates, "brand awareness" — and called it strategy. The practices that bought in aren't just behind on AI visibility. They've actively accumulated content that undermines their authority signals: generic, unverified, and structurally invisible to the engines now controlling patient recommendations. That's the hole the agency retainer model dug. And it's the hole a local AI authority engine exists to fill.
| Content Type | What AI Engines See | What Patients Experience | Trust Outcome |
|---|---|---|---|
| Generic AI batch content | Missing entity signals, no schema, no verifiable authorship — structurally invisible to citation logic | Reads like no real clinician was involved — confident-sounding but unverifiable | Trust destroyed before the first appointment |
| Keyword-stuffed agency posts | High word count, low Entity Trust — engines cross-reference and find nothing to anchor | Patients sense the absence of genuine clinical expertise — content feels hollow | Practice stays invisible in AI recommendations |
| AI Authority content with verified sourcing | Strong Entity Trust, Citation Velocity signals, and Semantic Density — engines find verifiable anchors throughout | Reads like a real expert who stands behind what they publish — structured, sourced, credible | Trust built; practice gets named as the single local answer |
| Content with schema and structured citations | Clear entity relationships and citation pathways — engines can trace claims back to authoritative sources | Patients encounter information that holds up under scrutiny — receipts, not vibes | Authority compounds with every published piece |
| Template-based agency deliverables (no clinical context) | Duplicate signals across dozens of clients — no differentiation, no local entity specificity | Indistinguishable from every other practice's content — nothing that earns trust or loyalty | Invisible to both engines and patients — worst possible outcome |
What AI Engines Actually Look for When They Decide to Trust a Practice
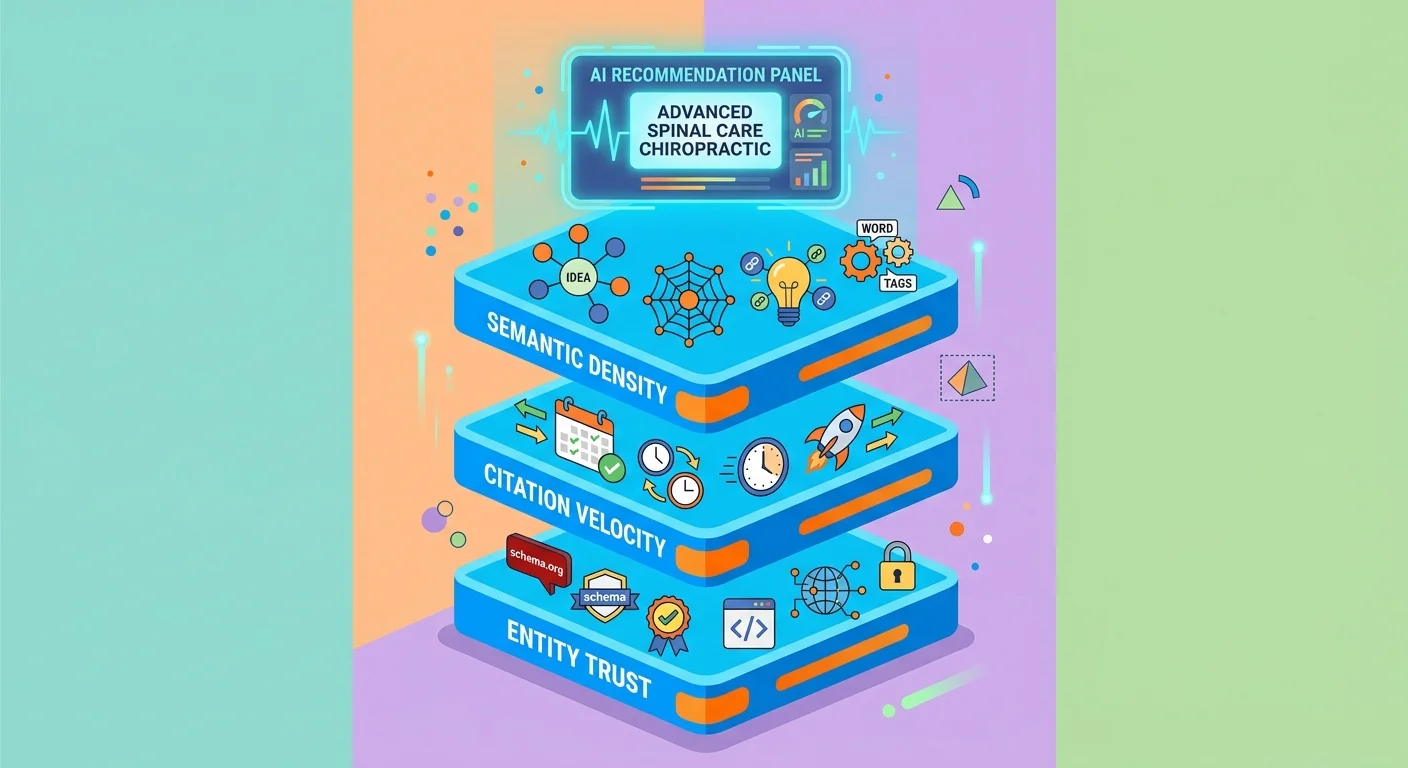
Here's the thing: AI engines don't care how polished your content sounds. They're not impressed by long-form articles that feel authoritative. They're not checking keyword density. Trust, to a generative engine, is structural. And it's built from three specific signals.
Those signals are Entity Trust, Citation Velocity, and Semantic Density. Every recommendation ChatGPT, Gemini, or Grok makes about a local provider runs through all three. Score well across them and you get named. Fall short on any one of them and you stay invisible — doesn't matter how many posts you've published or how much you've paid an agency to "build your brand."
Gartner predicts a 25% drop in traditional search engine volume by 2026. The citation decisions these engines make are already the most consequential moment in patient acquisition. Understanding what drives those decisions isn't optional. It's the whole game.
Entity Trust: The Foundation AI Engines Verify First
Entity Trust is the foundation. It's the engine's ability to confirm that a provider is who they say they are. The practice exists. It operates at a verified location. It holds the credentials it claims. Its information is consistent and structured across every platform where patients and engines go looking.
When an engine encounters a practice with mismatched NAP data, no schema markup, a thin Google Business Profile, and zero structured entity signals — it doesn't rank that practice lower. It doesn't name them at all. Entity Trust isn't a ranking factor. It's a prerequisite.
That's exactly where the agency retainer model broke down. Agencies built content. They didn't build entity infrastructure. So practices ended up with a library of published posts attached to a digital identity that generative engines can't verify. Every post. Every page. Structurally invisible. That's not a side effect of bad luck — that's the model doing exactly what it was built to do. Read how this model breaks down.
Citation Velocity: Why Consistent Publishing Compounds Authority
Citation Velocity is about what you do consistently — not what you launched once. Generative engines don't make one trust decision about a practice and walk away. They reassess. Constantly. The practices that keep publishing structured, verified AI Authority content compound their authority signals with every article. The ones that stop, erode. It's not a sprint. It's an asset that either builds or decays — there's no neutral.
Practices that publish a burst of content and stop are signaling that their authority isn't maintained. The engines notice. Consistent publishing isn't a volume play — it's a trust signal. Every receipt you add to the pile makes the next recommendation more likely. Every month you go dark, that pile erodes.
Semantic Density: How Depth of Coverage Signals Clinical Authority
Semantic Density is the one most practices don't even know exists. It's the depth of coverage across a topic — how thoroughly a practice has addressed the full range of clinical questions, conditions, and patient concerns in structured, sourced content. Not how much they've published. How deep they've gone.
An engine evaluating two chiropractors isn't just checking whether they've published something. It's evaluating whether they've covered the territory. The practice with ten interconnected AI Authority articles — structured properly, sourced correctly, cross-referenced for entity consistency — reads as the clinical authority. The practice with ten generic posts reads as noise. That distinction is Semantic Density. And it's exactly why receipts beat vibes every single time.
The Search Engine Journal analysis of generative citation architecture confirms it: generative engines construct structured citations dynamically via web trust indices. Semantic Density feeds those indices at the content level. Think of it as your receipt stack. The deeper it goes, the more territory you've covered — and the harder it gets for any competitor to knock you out of the recommendation.
| Trust Signal | What It Measures | How AI Engines Detect It | What Weak Execution Looks Like |
|---|---|---|---|
| Entity Trust | Whether a practice is who it claims to be — verified identity, credentials, location, and consistent structured data across every platform | Cross-referencing NAP consistency, schema markup, Google Business Profile completeness, and structured entity signals across directories and authoritative platforms | Mismatched business name or address across platforms, missing schema markup, thin or absent Google Business Profile, no structured credentials — the engine can't confirm the entity exists and won't name it |
| Citation Velocity | Whether a practice maintains a consistent, compounding record of structured authority content over time — not a one-time burst of publishing | Tracking the recency, regularity, and structural quality of published content — practices that publish and go dark signal that their authority isn't maintained | A library of old posts with no recent additions, inconsistent publishing gaps, content that lacks schema or sourcing — the engine treats the authority as stale and de-prioritizes the recommendation |
| Semantic Density | The depth and breadth of a practice's coverage across clinically relevant topics — how thoroughly a provider has addressed the questions real patients are asking | Evaluating whether interconnected AI Authority articles cover related conditions, patient concerns, and clinical questions in a structured, cross-referenced content network | A handful of isolated generic posts with no topical interconnection — the engine reads thin coverage as noise, not authority, and names the practice with the deeper receipt stack instead |
How the AI Authority Engine Turns Clinical Content Into Patient Trust at Scale

Entity Trust, Citation Velocity, and Semantic Density don't work independently. They stack. The practices building all three at a consistent publishing pace — with verified sourcing woven into every article — are the ones generative engines keep naming. The McKinsey report on the economic potential of generative AI projects $150 billion to $260 billion in annual economic value from generative AI applied to healthcare communication and productivity. That's not a technology stat. That's a trust infrastructure stat. The practices that build the infrastructure capture the value. The ones that don't hand it to whoever did.
More than 80% of healthcare consumers say access to peer-reviewed, factually validated patient education directly shapes their choice of clinician. That's not a preference. That's an instruction. Patients are already telling the industry exactly what moves the needle. Structured, sourced, entity-verified content published consistently — each article adding another receipt to the stack — is the answer to that instruction.
That's what shifting from agency retainers to an AI authority engine actually means in practice. Not a content upgrade. An infrastructure rebuild — one that turns a chiropractic practice's entire digital presence from a brochure AI ignores into a verified entity network generative engines actively cite.
Who This System Is Not For
This system isn't for everyone. That's not a caveat. It's a filter.
If you're expecting new patient bookings in 60 days, this isn't your system. Authority doesn't run on a microwave schedule. The practices that get the most out of this are the ones willing to build correctly and let it compound — not the ones chasing a 90-day miracle they'll abandon when the calendar runs out. If that's the frame you're operating in, start with what a healthy agency relationship looks like before going further.
And it's not for practices that want to run it themselves. The AI Authority Engine is a done-for-you infrastructure rebuild. The client does nothing beyond showing up as the clinical expert. If you want a system you can take over after a brief walkthrough, that's a different product. The practitioners who belong here are the ones already burned by the retainer model. Tired of paying for vibes. Ready to pay for receipts instead.
The Structural Anatomy of a High-Trust AI Authority Article
Every AI Authority article in the system follows the same verified architecture. It opens with a direct answer — clean, encyclopedic, structured so a generative engine can extract it and present it as a standalone citation. No warmup. No scene-setting. The answer first, backed by sourced data, every single time.
From there, the article builds outward — related conditions, patient concerns, clinical context — all cross-referenced to entity-verified information about the specific practice. Schema markup ties the content to the business entity. Internal linking builds the content network that tells engines this practice has covered the territory. Every layer is a receipt. Every receipt makes the next recommendation more likely.
That's what separates a practice that gets named from one that doesn't. It isn't magic. It isn't luck. It's receipts — stacked deliberately, published consistently, by a system that knows exactly what generative engines are checking. Patients trust receipts. Engines cite receipts. Practices that publish receipts get recommended. Practices publishing vibes stay invisible.
| Article Component | Why It Exists | What It Signals to AI Engines | What It Signals to Patients |
|---|---|---|---|
| Direct Answer Block | Gives generative engines a clean, extractable response to the exact clinical question a patient would type into ChatGPT or Gemini | Confirms the practice can directly answer a known patient query — making it a viable citation candidate for zero-click AI responses | Delivers the answer immediately, without burying it — building instant credibility with readers who are evaluating whether this practice knows what it's talking about |
| Schema Markup | Connects every article to the verified business entity — practice name, location, credentials, and service scope — in a structured format engines read directly | Closes the entity verification loop so the engine can confirm the content belongs to a real, specific, credentialed provider rather than an anonymous domain | Invisible to the reader but foundational to trust — it's the infrastructure that allows accurate, practice-specific information to appear consistently across AI platforms |
| Sourced Clinical Claims | Anchors every factual statement to a verifiable institutional or peer-reviewed source rather than leaving assertions ungrounded | Signals that the content meets the factual verification standard generative engines use when deciding what's safe to cite as a health recommendation | Demonstrates to the patient that the practice isn't publishing opinions — it's publishing receipts, which is exactly what healthcare consumers demand before trusting a clinician |
| Internal Content Network | Cross-references every article to related clinical questions, conditions, and patient concerns covered elsewhere in the practice's content library | Communicates Semantic Density — showing engines that this provider has covered the clinical territory, not just posted once and disappeared | Creates a cohesive educational experience where patients move naturally from one answered question to the next, deepening trust with every interaction |
| Consistent Publishing Cadence | Maintains Citation Velocity by adding verified, structured content to the practice's authority stack on a predictable, ongoing schedule | Signals that the practice's authority is actively maintained — not a one-time burst — which is the pattern engines reward with sustained citation priority | Reassures patients that the practice is current, engaged, and invested in their education — not a static brochure that was last updated years ago |
What Verified AI Authority Content Looks Like Versus What Most Practices Publish
Here's the thing most practices don't know: what you see when you look at your published content and what a generative engine sees are two completely different objects.
You see an article. The engine sees a document with no schema, no entity anchoring, no sourced claims, and zero structural signal that any of this was verified by someone who actually knows what they're talking about.
That gap isn't a ranking problem. It's an invisibility problem.
According to NIH data on patient web search behaviors, over 74% of patients use search engines and medical platforms to research symptoms and evaluate local clinical credentials before booking an appointment.
They aren't browsing. They're auditing.
And if what they find is a generic draft that reads like every other practice in your city — no sourcing, no structure, no signal that a real expert was ever involved — the engine doesn't cite it. The patient doesn't trust it. And the appointment never happens.
Verified AI Authority content doesn't look slightly better than what most practices publish. It looks structurally different.
The gap isn't topic selection. It isn't word count. It's the receipts.
Vibes-based content has none. Authority content is built on nothing but.
The Receipt Standard: What 'We Don't Publish Vibes' Actually Means in Practice
When iTech Valet says "we don't publish vibes, we publish receipts" — that's not branding. It's a structural description of how every article gets built.
A receipt is a verifiable, sourced, entity-anchored claim. It's the kind of signal that tells a generative engine this information is trustworthy enough to cite and pass on to a patient asking a clinical question.
Not a well-written paragraph. Not a topic covered with confidence. A claim that can be checked — and holds up when it is.
The Pew Research Center study on clinical AI trust found that approximately 60% of U.S. adults are uncomfortable with healthcare providers relying on AI for their medical care.
That discomfort doesn't come from AI existing. It comes from AI content that feels unverifiable — smooth-sounding claims with nothing behind them.
Receipts dissolve that. When a patient reads an article that leads with a direct clinical answer, backs it with sourced data, and connects that content to a verified local practice, something shifts. They don't feel like they're reading AI output. They feel like they found the expert. That's not a perception trick. That's what structured authority content actually does.
More than 80% of healthcare consumers say access to peer-reviewed, factually validated patient education directly shapes their choice of clinician.
That's the receipt standard at work.
The practices capturing those patients aren't out-publishing everyone else. They're publishing differently — structured, sourced, entity-verified documents that a generative engine can extract from, a patient can trust, and a clinician can stand behind.
How to Audit Your Current Content Against the AI Trust Standard
Here's the audit. One honest question: if you stripped your practice name off every article you've published, would a generative engine have any reason to trust what's left?
No entity signals. No schema. No sourced claims. No cross-referencing to verified clinical credentials.
What most practices find when they run that check isn't a content gap. It's a complete absence of infrastructure. Topics published. Authority not built.
The NIH data on patient web search behaviors puts over 74% of patients online before their first appointment. That makes this a direct revenue question — not a content quality debate.
Every article that fails the receipt standard is a patient encounter that never happened. Every month that content stays live, it's not just underperforming — it's actively signaling to generative engines that no real expert was involved.
If an agency built your content library and you're not sure whether it meets this standard, that uncertainty is the answer. the vetting criteria
- Does each article lead with a direct, encyclopedic answer to a specific patient question?
- Are any claims sourced to verified external authorities — not just asserted confidently?
- Does schema connect the content to your verified practice entity?
- Do internal links build a content network — or just sit there in isolation?
| Content Attribute | Commodity AI Draft | AI Authority Article | Why the Difference Matters |
|---|---|---|---|
| Opening Structure | Begins with context-setting, background, or a general introduction to the topic | Leads immediately with a direct, encyclopedic answer to the specific patient question — no preamble, no scene-setting | Generative engines extract first-paragraph answers. If the answer isn't there, the article isn't cited. |
| Claim Sourcing | Assertions are stated without attribution — no external sources, no institutional verification | Every clinical or factual claim is sourced to a verified external authority and marked with a citation signal | Unsourced content is invisible to AI trust scoring. Receipts — sourced, verifiable claims — are what engines look for. |
| Entity Anchoring | Content floats in isolation — no connection to the practice's verified business entity or local credentials | Schema markup and internal linking tie every article back to the practice's verified Entity Trust profile | Without entity anchoring, a generative engine can't confirm the source is real. The content exists; the recommender doesn't. |
| Semantic Depth | Covers a single surface-level topic with no cross-referencing to related conditions, questions, or patient concerns | Builds Semantic Density across related topics, patient scenarios, and clinical context — a content network, not a standalone post | AI engines reward content breadth that proves a practice has covered the territory. A single article isn't authority. A network is. |
| Citation Velocity Signal | Published once and left static — no consistent publishing cadence, no compounding authority signal | Part of a consistent publishing system that builds Citation Velocity over time — each article strengthens the next | Authority compounds. A single well-built article helps. A system of them tells every engine this practice is the ongoing expert. |
| Patient Trust Outcome | Reads like generic AI output — indistinguishable from every other practice in the market | Reads like a verified expert answered a real patient question — sourced, structured, and connected to a credentialed local practice | Patients don't trust AI content. They trust receipts. The article that reads like a receipt gets the appointment. |
Frequently Asked Questions About AI Authority Content and Patient Trust
Good. The structural case is done. Now come the questions practitioners ask after they've already been burned — the ones nobody asks until they've already paid for something that didn't work.
Five questions. Direct answers.
How does AI authority content build patient trust rather than alienating them?
That 60% discomfort number isn't a case against AI content. It's a case against bad AI content.
Patients aren't rejecting AI-assisted information. They're rejecting content that feels unverifiable — generic output with no identity behind it, untethered from any real clinical voice. AI Authority content does the opposite. It leads with a direct answer to a specific patient question. It backs that answer with sourced data. It connects to a verified practice entity through schema and internal linking.
When a patient reads that, they don't feel like they found a content farm. They feel like they found the expert.
More than 80% of healthcare consumers say validated patient education directly shapes their choice of clinician. That's not a soft trend. That's what receipts do — and it's exactly why the trust barrier doesn't kill the strategy. It confirms it.
Why do generic AI blog posts fail to satisfy generative engine standards?
Because they produce topics without infrastructure.
A generative engine doesn't evaluate your article the way a human reader does. It's checking for verifiable web trust indices — entity signals, schema anchoring, sourced claims traceable to authoritative external sources, cross-referencing to a verified business entity. Most generic AI output has none of that. It's a document that covers a topic and nothing else.
Conversational engines construct citations dynamically. They pull from content that signals trustworthiness — not content that fills a word count. Generic drafts don't signal anything.
They're invisible to the engine. Forgettable to the patient. And actively harmful to the practice that published them.
What makes patient-facing clinical content readable and authoritative to both humans and AI engines?
Here's what most people get wrong: they treat "readable to patients" and "trustworthy to AI engines" like two separate problems. They're not.
Start with the direct answer — the specific clinical question a patient would actually ask, answered immediately in plain language. No preamble. Build from there: related conditions, clinical context, the practice's specific area of expertise. Short paragraphs. Source every claim that deserves a source. Write like the expert explaining it directly — not like someone fulfilling a content brief.
Do that, and the engine sees structured, entity-anchored content worth citing. The patient sees a clinician who actually knows what they're talking about.
Same standard. Same execution. One receipt — two audiences convinced.
How do structural citations and schema play a role in deepening patient trust on AI platforms?
Schema and citations aren't decoration. They're the connective tissue between what you publish and what an engine trusts.
Schema markup tells the engine who you are: your practice name, location, credentials, the entity behind the content. Structural citations tell it your claims are backed by verifiable external authorities — not internal opinion. Generative engines construct recommendations based on verifiable web trust indices, and schema is a primary input into that index.
Without it, your content is an anonymous document. With it, it's a verified, entity-anchored asset a generative engine can confidently attach to a local recommendation.
Patients feel the difference without knowing why. The content just reads as more authoritative. That feeling isn't perception. That's schema working correctly — and it's exactly the kind of receipt that gets a practice named.
Can an AI Visibility Check reveal why patients are finding my local competitors instead of me?
Yes. And it's usually the fastest way to make the problem impossible to rationalize away.
Gartner projects a 25% drop in traditional search volume by 2026 as patients shift to conversational AI agents for local health recommendations. That shift isn't coming — it's already happening. The AI Visibility Check surfaces exactly what ChatGPT, Gemini, and Grok say when someone in your market asks for a recommendation right now.
Most practitioners who run it find one of two things: the engine names a competitor, or it returns a generic answer that doesn't include them at all. Neither outcome is a data problem. Both are authority infrastructure problems.
Seeing it in real time changes the conversation. It's not an abstract argument about AI trends anymore. It's your market, your competitors, your name — either in the answer or not.
The check takes 15 minutes. What it reveals usually takes much longer to build back.
The Receipt Is the Strategy
Here's the verdict.
Patients don't trust AI content. They trust receipts. The practices publishing receipts — structured, sourced, entity-anchored — are the ones generative engines name when someone asks who the best chiropractor in their area is.
The ones publishing vibes stay invisible. That gap isn't closing on its own.
The receipt metaphor isn't a branding choice. It's a structural description of what actually has to get built.
Entity Trust tells the engine who you are. Citation Velocity tells it you've consistently covered the territory. Semantic Density tells it your content is deep enough to be worth citing to a patient with a real clinical question.
Stack all three — consistently, over time — and you don't have a content library. You have authority infrastructure. That's what the local AI authority engine builds: not a beautiful brochure AI can't read, but a verified entity network generative engines actively cite as the local answer.
The practices winning this aren't waiting to see if AI search is real. They're already building.
Every month of execution compounds. Every article is another receipt in the stack. And every month a competitor keeps going while you wait is a month of authority they've built that you haven't.
iTech Valet's position is simple: the businesses that aren't the answer are invisible. Receipts, not vibes — that's the whole game. And it starts the moment you decide you'd rather be named than overlooked.
You've seen the argument. You know the standard. Now the only question is whether your name is in the answer — or someone else's is.
621 Enterprises, Inc. | Copyright 2026 | All rights reserved