
The AI Content Paradigm Shift: Why AI Authority Articles Have Replaced Blogging for Healthcare Practices in 2026
AI Authority articles have replaced traditional blogging for healthcare practices because AI engines do not return lists. They return a verdict.
When a patient asks ChatGPT or Gemini who the best chiropractor near them is, one name comes back. Not ten links. Not a directory. One answer. The practices earning that answer are not the ones with the most content. They are the ones with the most machine-readable authority infrastructure.
Traditional blogging was built for a different world. A patient typed a keyword, got a ranked list, and picked someone. That model is collapsing. Gartner projects a 25% drop in traditional search engine volume by 2026 as users migrate to conversational AI interfaces. The mechanism driving patient discovery has already changed.
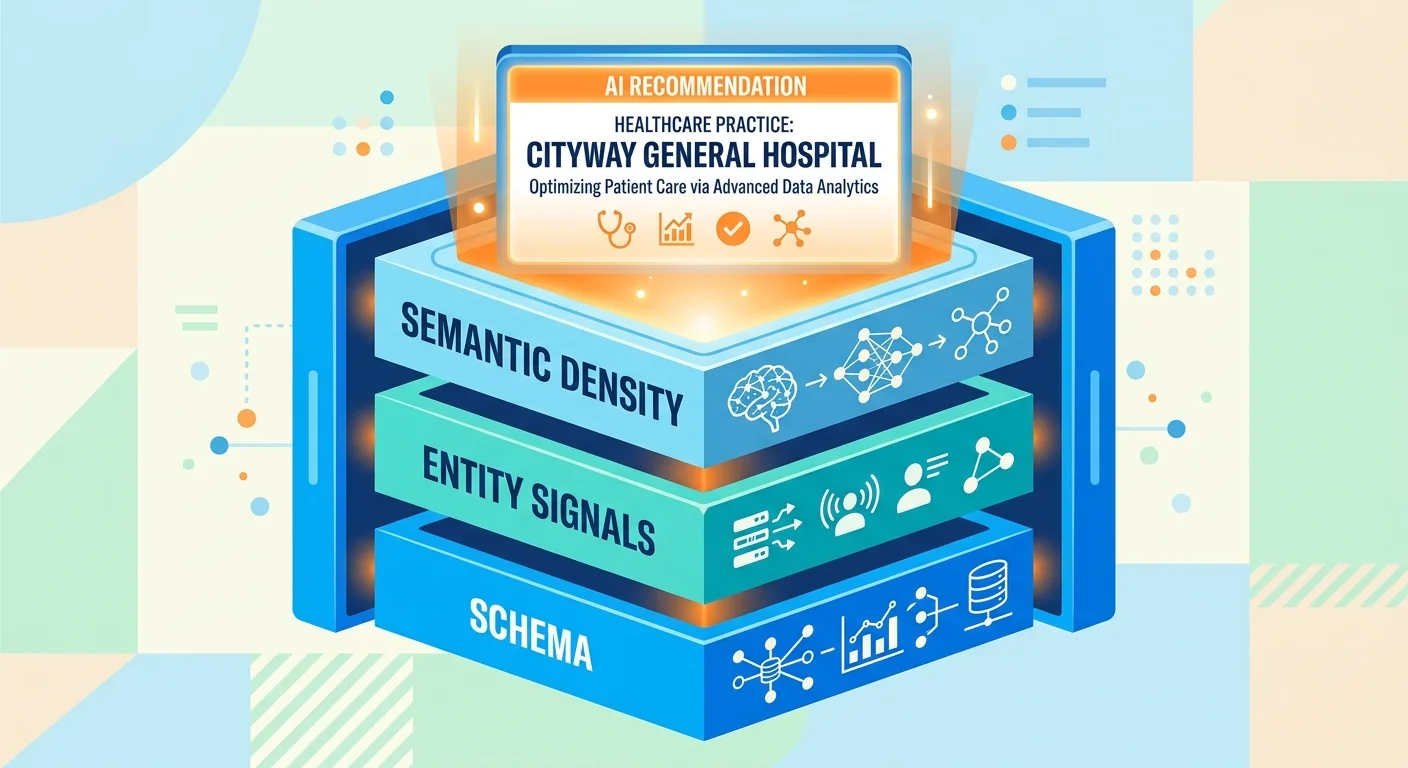
Conversational AI engines evaluate healthcare providers through three structural signals: Schema, Entity Signals, and Semantic Density. Schema tells an AI engine what a practice is and what it treats. Entity Signals confirm the practice is verified and trustworthy — cross-referenced across directories, citations, and structured data. Semantic Density signals genuine topical depth, not surface-level content. Blogging builds none of these systematically. AI Authority articles are engineered specifically to build all three.
60% of U.S. adults now recognize AI in their everyday platforms, and healthcare patients are no exception. Conversational AI models are actively changing how patients evaluate and select local clinical providers. Practices still investing in standard content production without authority infrastructure are investing in a format patient discovery no longer prioritizes.
The shift is not coming. It is already here. Healthcare practices that realign their content strategy around AI Authority articles — and the Schema, Entity Signals, and Semantic Density those articles reinforce — become the verdict AI delivers. Practices that do not become invisible.
Last Updated: July 10, 2026
- • From Directory Entry to Verdict: How AI Engines Actually Deliver Healthcare Recommendations
- • The Machine-Readable Authority Stack: How AI Engines Evaluate Healthcare Providers
- • What AI Authority Articles Are and How They Differ From Traditional Blog Posts
- • How to Audit and Transition Your Healthcare Content From Blogging to AEO Execution
-
• Frequently Asked Questions
- • Why has traditional blog post writing stopped producing new patients for healthcare practices in 2026?
- • How do conversational AI engines decide which local clinic or chiropractor to recommend?
- • What is the difference between traditional SEO and Answer Engine Optimization (AEO) for healthcare practices?
- • What are the compliance and accuracy risks of using commodity AI content mills for healthcare content?
- • How long does it take for AI Authority articles to start building measurable entity trust?
- • Can a healthcare practice retrofit its existing content library into AI Authority articles, or does everything need to be rebuilt from scratch?
- • The Verdict Is Already Being Delivered — Is Your Name In It?
From Directory Entry to Verdict: How AI Engines Actually Deliver Healthcare Recommendations

Think about how a courtroom works. The jury doesn't hand you a list of suspects and wish you luck. They deliver a verdict. That is exactly what conversational AI does.
Traditional search handed patients a directory. Ten blue links, a map pack, a few ads — and the patient did all the filtering. AI engines cut that step entirely. They weigh every available signal, build a confidence score, and name one answer.
That mechanism matters more than most practice owners realize. If you don't understand how AI engines reach their verdicts, every content decision you make is aimed at the wrong target.
The Shift From Search Lists to Single Answers
Gartner projects a 25% drop in traditional search engine volume by 2026 as users migrate to conversational interfaces. That's not a distant forecast. That transition is already running through the patient discovery channel right now.
Here's the thing — 60% of U.S. adults already recognize AI in their everyday platforms, according to Pew Research Center. Healthcare patients aren't some separate category. They are those adults. Searching for a chiropractor, a physical therapist, a primary care provider. And a growing share of them are typing that question into ChatGPT or Gemini instead of Google. The platform shift isn't theoretical. It's the waiting room of the practice down the street.
So when a patient asks an AI engine who to see — the engine doesn't serve options. It serves a name. And that name isn't the practice with the most blog posts. It's the one whose authority infrastructure — Schema, Entity Signals, and Semantic Density — gave the engine enough structured trust to make a confident call. Content volume isn't the input. Verified, machine-readable authority is.
Why Traditional Healthcare Blogging No Longer Converts Searches Into Patients
Traditional healthcare content was built for a completely different job. Rank in a list. Attract a click. Hope the patient stayed long enough to book. That entire chain assumed a human was doing the filtering. AI engines don't filter. They decide.
And a standard healthcare article optimized for keyword density gives an AI engine almost nothing it can use. It doesn't confirm the practice's entity. It doesn't establish verified credentials. It doesn't demonstrate topical depth across the clinical areas the practice actually treats. What it does produce is authority visibility — for a system that no longer governs how patients find care.
Practices asking why their AI Authority articles aren't moving the needle almost always find the same root problem. The content was built for the wrong output. Writing for a human reader who clicked through a list is a fundamentally different task than building machine-readable authority that earns a verdict. Same words on a screen. Completely different jobs.
Why Keyword-First Content Fails the AI Verdict Test
Keyword-first content starts with the wrong question. The old question was: what does a patient type into a search bar? The right question — the one that governs AI recommendations — is: what does an AI engine need to trust this practice enough to name it?
Those aren't variations of the same question. One optimizes for a string of text. The other optimizes for a web of structured, verified, machine-readable entity signals. Keyword density and click-through-rate link patterns are irrelevant inputs to an AI engine rendering a verdict.
AI engines aren't reading your content and thinking about search intent. They're evaluating whether your entity is credible enough to stake their recommendation on. Schema, Entity Signals, and Semantic Density answer that question. Keywords don't.
| Discovery Model | What the Patient Sees | Content Format That Wins | Role of the Provider |
|---|---|---|---|
| Traditional Search (Google) | A ranked list of ten or more options — map pack, organic results, paid ads — requiring the patient to evaluate and choose | Keyword-optimized articles and directory listings built to rank in a list and attract a click | One of many options competing for a click — the patient does the filtering |
| Conversational AI (ChatGPT, Gemini, Grok) | A single named recommendation delivered as a confident verdict — no list, no alternatives offered | AI Authority articles built on Schema, Entity Signals, and Semantic Density that give the engine structured trust signals | The sole recommended answer — the engine does the deciding, and the practice either earns the verdict or is invisible |
| Directory Listings (Yelp, Healthgrades, Zocdoc) | A filtered category page with multiple providers sorted by rating, distance, or relevance | Complete, accurate structured profiles with verified credentials and consistent entity data across platforms | A candidate among many — patients still make the final choice from a presented set |
| AI-Assisted Decision (voice search, AI summaries) | A spoken or embedded recommendation with zero visual alternatives — the engine names one practice and stops | Machine-readable authority infrastructure that confirms the practice entity across Schema, Entity Signals, and Semantic Density | The answer the engine stakes its credibility on — practices without authority infrastructure are not considered |
The Machine-Readable Authority Stack: How AI Engines Evaluate Healthcare Providers
AI engines do not read your content the way a patient does.
They evaluate your entity the way a court evaluates a witness. Looking for corroboration. Structure. Verified credentials. Before they stake their recommendation on your name.
McKinsey's research on AI adoption makes it plain — professional services are accelerating through digital transformation at a pace that leaves laggards behind permanently. Healthcare is not ahead of that curve. It is inside it. And the practices pulling ahead are not publishing more blog posts. They are building the machine-readable infrastructure that AI engines actually use to make decisions.
That infrastructure has three layers: Schema, Entity Signals, and Semantic Density.
Together, they form the authority stack an AI engine reads before it decides whether a practice is worth naming. Know all three, and you understand the difference between being a possibility and being the verdict.
Schema, Entity Signals, and Semantic Density: The Three Pillars AI Uses to Rank Trust
Schema is the foundation. It is structured data embedded directly in a practice's digital presence — machine-readable language that tells AI engines who the practice is, what it treats, where it operates, and what credentials it holds.
Without Schema, an AI engine is guessing. And guesses do not become verdicts. With Schema, the engine has a verified identity it can stake a recommendation on. That is not a minor technical detail. That is the difference between being named and being skipped.
Entity Signals go a layer deeper. Cross-referenced confirmations — directory listings, citations, structured mentions across authoritative platforms — tell AI engines a practice is real, consistent, and trusted by verified sources beyond its own website. Published analysis on conversational healthcare from the National Institutes of Health confirms that patients are filtering provider recommendations through conversational AI interfaces at a growing rate. Entity Signals are what give those interfaces the confidence to name one practice over another. Inconsistent listings do not just look sloppy. They actively destroy the authority signal an AI engine needs to commit to a recommendation.
Semantic Density is where most healthcare practices fall apart. Not because they lack content — because their content lacks depth.
An AI engine evaluating a chiropractor for a patient query is looking for evidence of genuine subject-matter authority across the clinical areas the practice actually treats. Surface-level articles scattered across loosely related topics do not produce that signal. That gap is exactly what separates content built to function as an AI Authority article from a standard keyword post. Same screen. Completely different jobs.
What a Structurally Invisible Healthcare Website Looks Like to an AI Engine
Here is what structural invisibility looks like in practice.
An AI engine queries a local market for a chiropractor. It finds a practice with a well-designed site, years of published articles, and a functioning booking system. It also finds no Schema markup, inconsistent directory listings, and content that touches dozens of topics without demonstrating depth in any of them.
The engine cannot confirm the entity. It moves on. The practice never knew it was evaluated — and never understood why the phone stopped ringing.
The Local AI Authority Engine is built specifically to close that gap — constructing the full authority stack from Schema through Entity Signals to Semantic Density.
A practice without that stack is not competing for the recommendation. It is invisible to the process entirely.
| Authority Signal | What AI Engines Look For | Blogging Score | AI Authority Article Score |
|---|---|---|---|
| Schema | Structured data confirming practice identity, service areas, credentials, and location in machine-readable format | Absent — standard articles contain no embedded Schema markup | Built-in — every AI Authority article reinforces structured Schema signals across the practice's digital presence |
| Entity Signals | Cross-referenced citations and directory listings that verify the practice is real, consistent, and trusted by authoritative third-party sources | Weak — articles generate no cross-platform entity corroboration | Strong — AI Authority articles are architected to reinforce entity consistency across verified platforms |
| Semantic Density | Demonstrated topical depth across the clinical areas the practice actually treats — not surface-level coverage of loosely related subjects | Shallow — blogging produces volume without verifiable subject-matter authority in any defined clinical area | Deep — each AI Authority article builds compounding depth in the practice's core clinical territory |
| Credential Verification | Confirmable professional credentials and institutional affiliations the AI engine can validate against authoritative sources | Not addressed — standard content formats have no mechanism for embedding verified credential data | Addressed — credential signals are structured into the authority infrastructure from the foundation up |
| Topical Consistency | A coherent, non-contradictory body of content that signals the practice is the authoritative source on a defined set of clinical topics | Inconsistent — broad topic coverage across unrelated subjects dilutes authority rather than concentrating it | Consistent — AI Authority articles are mapped to a defined semantic cluster that concentrates authority in the practice's actual specialty |
What AI Authority Articles Are and How They Differ From Traditional Blog Posts
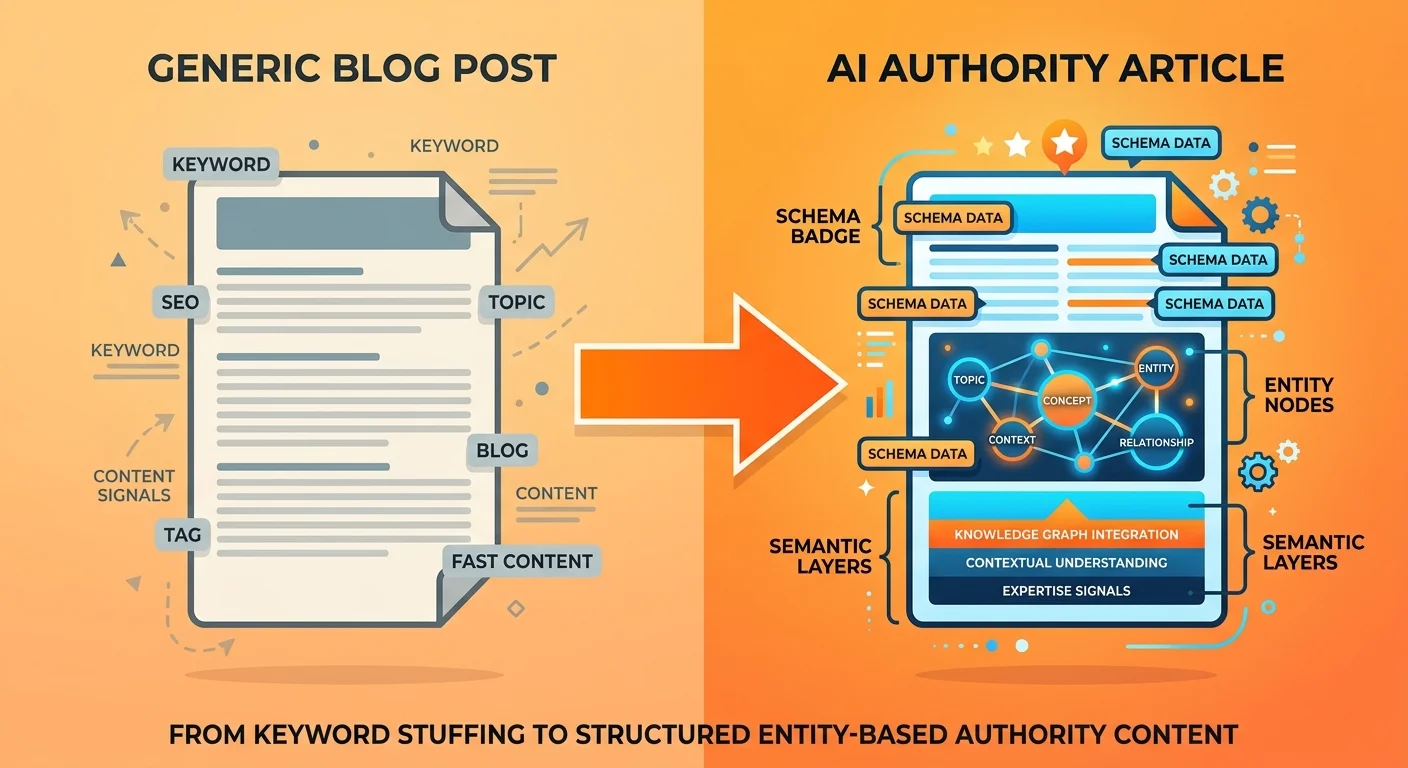
An AI Authority article is not a better blog post.
It is a different object entirely. Different reader. Different evaluator. Different job.
Traditional blog posts were written for humans scrolling a ranked list. The goal was a click. Hold attention. Hope they booked. Every decision in that format assumed a human was doing the filtering.
AI engines do not filter. They decide. And the side-by-side structural contrast between these two formats makes that gap impossible to minimize — one chases a click, the other earns a verdict.
AI Authority articles are engineered for machine-readable evaluation. Every element — Schema markup, entity confirmations, topical depth — exists to answer one question: does this practice carry enough structured authority for an AI engine to stake its recommendation on it?
Gartner projects a 25% decline in traditional search volume by 2026. That is not a warning. That is a description of what is already happening in the patient discovery channel. Patients stopped waiting for a list. They are asking for a name. AI Authority articles are what put a practice's name in that answer.
The Structural Anatomy of an AI Authority Article
The structure of an AI Authority article is not cosmetic. It is functional.
Every layer has a specific job. Schema. Entity Signals. Semantic Density. None of it is decoration. All of it is load-bearing.
Schema anchors the article to a verified entity. It tells the AI engine who wrote this, what practice it represents, what credentials that practice holds, and what clinical territory it covers.
Without it, the article is anonymous content in an unverified namespace. The engine cannot attach it to a trusted source. And content the engine cannot verify does not become the verdict.
Entity Signals and Semantic Density stack on top of that foundation. A properly built AI Authority article reinforces cross-platform entity consistency — same credentials, same service area, same clinical focus as every directory listing and citation tied to the practice. No contradictions. No gaps. The engine reads a coherent, verifiable picture and trusts what it finds.
Then there is topical depth. Not surface-level keyword coverage. Actual subject-matter authority across the clinical areas the practice treats. That depth is what separates a trusted entity from the commodity content AI engines already know to discount.
AEO Content Writing Services exist specifically to build that depth systematically — not as isolated pieces, but as a compounding authority infrastructure that gets stronger every month.
Who This Approach Is Not For
Here's the thing — this approach is not for every healthcare practice.
That is not a disclaimer. That is a filter.
If you want a content mill producing high-volume articles at low cost, this is not that. If you need measurable ROI in 90 days, this is not that. If you are looking for a shortcut that replicates the authority stack without actually building it — that shortcut does not exist.
Any agency telling you otherwise is selling you a version of the hopium that has already failed you once.
The FTC enforces actively against ungrounded AI performance claims. Hollow promises about AI visibility are not just a disappointment — they are a documented liability under current regulatory guidance. Any agency selling you guaranteed rankings or 90-day AI dominance is not just wrong. They are exposed.
AI Authority articles built to the standard described here are the alternative to that risk. But they require a practice willing to treat authority as a compounding asset — not a monthly line item that has to justify itself in 30-day windows.
If that is not your decision framework right now, this is not the right moment. Come back when it is.
| Element | Traditional Blog Post | AI Authority Article | Why It Matters for AI Recommendations |
|---|---|---|---|
| Primary Purpose | Attract a human reader through search; hold attention long enough to earn a click or booking | Build machine-readable authority signals that earn a confident AI recommendation verdict | AI engines evaluate entity trust, not reader engagement — the purpose of the content determines whether it registers at all |
| Structural Foundation | Keyword density, meta descriptions, and internal linking patterns optimized for click-through rates | Schema markup, Entity Signals, and Semantic Density layered into a verified authority stack | Without structured Schema and entity confirmation, an AI engine cannot attach the content to a trusted, identifiable source |
| Content Depth Model | Surface-level coverage of multiple keyword clusters to maximize topic reach and search visibility | Demonstrated topical depth within the clinical areas the practice actually treats — precision over volume | AI engines discount broad, shallow content libraries; they reward genuine subject-matter authority in a defined clinical territory |
| Entity Verification | No cross-platform consistency requirement; directory listings, credentials, and service area may differ across sources | Content reinforces and confirms the same credentials, service area, and clinical focus across every authoritative platform | Inconsistent entity signals force an AI engine to move on — consistent cross-platform confirmation gives it the confidence to name one practice over another |
| Asset Behavior Over Time | Depreciates as search algorithms shift; value tied to keyword ranking windows that can disappear overnight | Compounds as authority signals accumulate — each article reinforces and deepens the entity trust established by the last | AI engines build trust incrementally; a compounding authority stack becomes harder to displace the longer it runs |
| Output Delivered to the Patient | A ranked list of possible providers the patient must evaluate and choose between | A single named verdict — the practice the AI engine trusts enough to stake its recommendation on | Patients asking conversational AI engines are not browsing a list; they are receiving a decision — one practice gets named, the rest are invisible |
How to Audit and Transition Your Healthcare Content From Blogging to AEO Execution
So you know what AI Authority articles are.
Harder question: what happens to everything you've already published?
Most practices have years of content sitting live right now. Some of it is worth keeping. Most of it isn't.
The audit tells you which is which. Skip it, and you burn time retrofitting articles that were never going to earn a verdict — content the engine ignores no matter how many times you update it.
This isn't a content refresh.
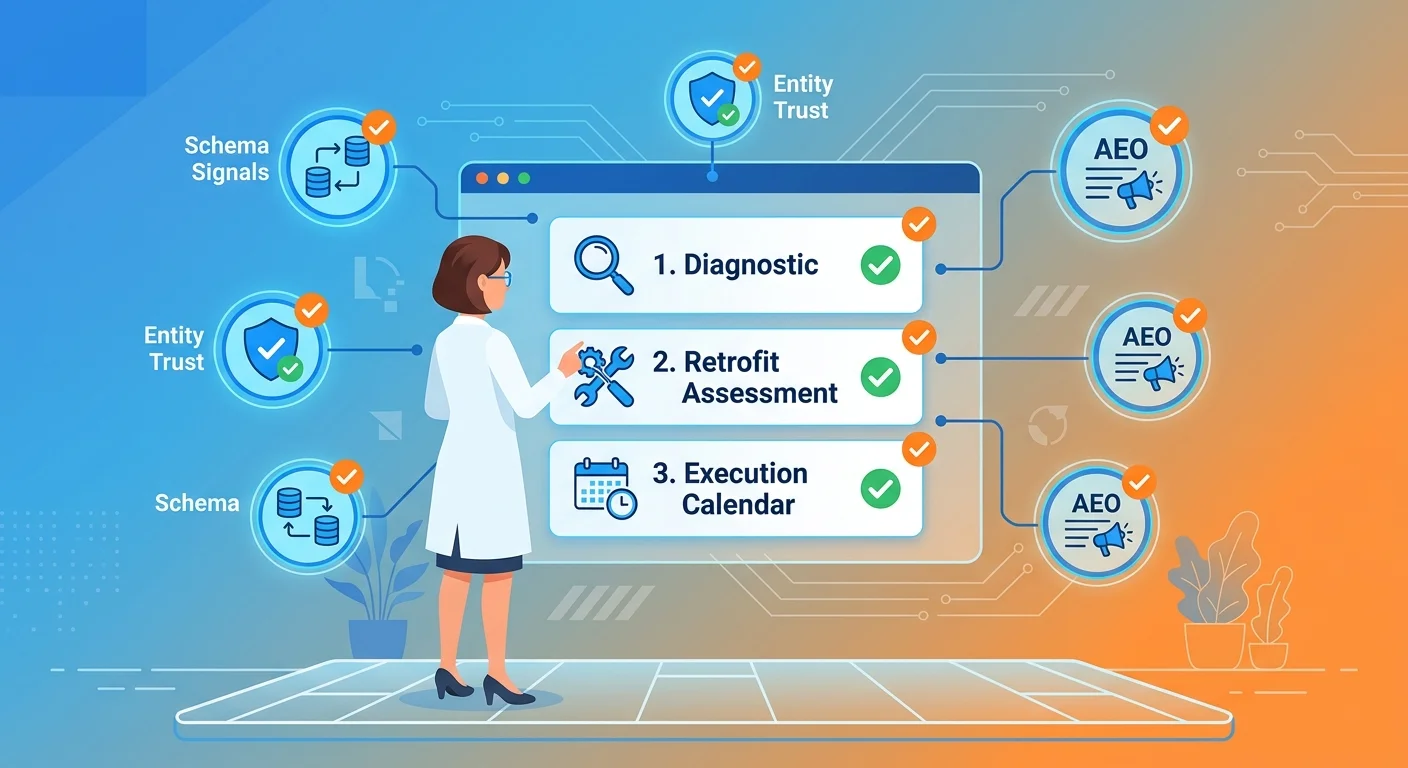
It's a structural rebuild. Three steps. Clear sequence. No guessing.
Step 1 — Run an AI Visibility Diagnostic on Your Current Content
This is the step most practices skip entirely.
Before anything gets written, retrofitted, or rebuilt — you need to know what AI engines actually see when they evaluate your current content. Not a traffic report. Not a keyword snapshot. A structured assessment of whether your existing content carries the Schema, Entity Signals, and Semantic Density that AI engines use to render a verdict.
Pew Research Center found that more than 60% of U.S. adults already recognize AI in their everyday technology. Their expectations have shifted. They're not scanning a list. They're asking for a name.
That shift makes the diagnostic non-optional. A practice with no baseline has no way to measure the gap — and no way to close it.
The AI Visibility Check is where this starts — a structured look at what ChatGPT, Gemini, and Grok actually return when someone asks for a provider recommendation in your market.
The results make the problem real. The gap between what AI engines currently see and what they need to see is exactly the scope of work that follows.
Step 2 — Identify Which Content Can Be Retrofitted and What Must Be Rebuilt
The diagnostic produces two categories.
The first has real topical depth, accurate clinical information, and a structural foundation worth upgrading — Schema added, Entity Signals reinforced, Semantic Density expanded. The second was written to hit a keyword target. No clinical specificity. No authority signals worth preserving.
That second category doesn't get retrofitted. It gets replaced.
The decision rule isn't sentimental.
Content that amplifies a practice's clinical voice and reinforces entity trust across AI platforms is worth investing in. Content written to hit a keyword target and nothing else is dead weight.
SEC regulatory guidance on AI disclosure made clear that accuracy and verifiability are the standards governing how AI-cited content is evaluated institutionally. Content that can't meet that standard has no place in an authority infrastructure.
Step 3 — Build the AEO Content Execution Calendar
The execution calendar is where intent becomes infrastructure.
Not a content schedule. A sequenced build — each AI Authority article layering additional Semantic Density onto the foundation the articles before it established.
The calendar is built around clinical territories, not keyword clusters.
A practice treating three distinct conditions needs genuine depth in all three. Not one pillar article per condition — a full cluster of AI Authority articles demonstrating subject-matter authority in each territory.
That depth is what AI engines evaluate when they decide whether a practice has earned the right to be named.
This is the methodology Gerek Allen built at iTech Valet — a structured asset roadmap that sequences content to compound rather than accumulate.
Practices that follow it don't produce more content. They produce the right content, in the right order, with every article reinforcing the entity trust the previous one established.
That's the difference between a content library and an authority infrastructure.
| Audit Category | What to Check | Blogging Red Flag | AEO Upgrade Action |
|---|---|---|---|
| Schema Structure | Does the content carry structured data identifying the practice entity, author credentials, service area, and clinical specialties? | No schema markup present — content is anonymous to AI engines with no verifiable entity attachment | Add FAQPage, MedicalBusiness, and Person schema; anchor every article to a verified practice entity with confirmed credentials and service territory |
| Entity Signal Consistency | Does the content confirm the same practice name, address, specialties, and clinical focus as the practice's directory listings and cross-platform profiles? | Content contradicts or ignores directory data — AI engines detect inconsistency and cannot confidently attach the content to a trusted source | Audit every entity signal against NAP data, directory profiles, and clinical descriptions; rewrite any content that introduces contradictions or gaps |
| Semantic Density | Does the content demonstrate genuine clinical depth — specific conditions treated, mechanisms explained, patient outcomes addressed — or does it skim surface-level topics? | Content was written to hit keyword volume targets with no clinical specificity — AI engines classify it as commodity content and discount its authority value | Rebuild low-depth articles as full AI Authority articles with condition-specific clinical voice, topical clusters, and Semantic Density that demonstrates real subject-matter authority |
| Topical Coverage Architecture | Is the content organized around complete clinical territories — each condition addressed with a full cluster of supporting articles — or scattered across unrelated keyword opportunities? | Content library is a collection of disconnected articles chasing individual keywords with no cluster architecture reinforcing any clinical territory | Map the practice's core clinical territories and sequence a full AI Authority article cluster for each — every article reinforcing the entity trust the previous one established |
| Accuracy and Verifiability | Can every clinical claim in the content be verified against institutional sources — peer-reviewed literature, professional guidelines, or credentialed clinical standards? | Content contains generalized health claims with no sourcing — unverifiable assertions that institutional AI evaluation standards treat as a liability, not an authority signal | Replace unverifiable claims with sourced, institutionally grounded clinical statements; every factual assertion must trace to a verifiable authority that AI engines recognize as trustworthy |
| Content Classification Decision | Based on the audit above, does the article demonstrate enough genuine clinical voice, structural integrity, and entity alignment to justify an AEO upgrade — or was it built purely for keyword placement? | Content was written entirely for keyword placement with no clinical specificity, no entity signals, and no structural foundation worth preserving | Retain and upgrade articles with genuine clinical depth; replace keyword-only content entirely — retrofitting articles with no authority foundation wastes resources that compound better when invested in new AI Authority articles |
Frequently Asked Questions
Here's the thing — every practice asks some version of these questions before they move. Get the answers wrong and a competitor earns the verdict instead.
These aren't hypothetical. They're the exact objections that either get resolved or become the reason a practice waits too long.
Why has traditional blog post writing stopped producing new patients for healthcare practices in 2026?
Traditional content was built for a ranked-list world. Every format decision — keyword placement, broad topic coverage, clickable headlines — was engineered to land a position in Google's results and then convince a human to click.
AI engines don't produce a ranked list. They deliver a verdict.
A standard blog post carries no Schema, no verified Entity Signals, no Semantic Density. There's nothing in that format for an AI engine to evaluate. The engine scans for structured trust signals, finds none, and moves to the next practice.
The patient shifted to asking. The content never shifted to answering at the machine-readable level that earns a recommendation. That's why the bookings stopped.
How do conversational AI engines decide which local clinic or chiropractor to recommend?
Three things. Whether the entity is verified. Whether the authority claim is consistent across platforms. Whether the content demonstrates genuine clinical depth.
A practice with complete Schema, consistent Entity Signals across directories and structured data, and a library of AI Authority articles covering its clinical territories with real specificity — that practice earns the recommendation.
A practice with a polished site and a backlink profile earns nothing from an AI engine. The engine is not reading your site. It is reading the trust infrastructure you either built or did not build.
There is no shortcut through that evaluation. The engine either finds the authority signals or it moves on.
What is the difference between traditional SEO and Answer Engine Optimization (AEO) for healthcare practices?
Traditional SEO optimizes for a ranked list. AEO optimizes for a single verdict. Those are not variations of the same strategy — they are different models built for different engines.
Traditional SEO targets keyword density, backlink volume, and page authority scores. AEO targets Schema completeness, Entity Signal consistency, and Semantic Density across a clinical territory.
The output of traditional SEO is a position on a list that patients now skip. The output of AEO is a name in the answer AI delivers when a patient asks who to trust.
Practices still investing in traditional SEO in 2026 are optimizing for a channel their patients already left.
What are the compliance and accuracy risks of using commodity AI content mills for healthcare content?
The risk isn't theoretical. The FTC actively enforces against businesses making false or ungrounded claims about AI accuracy — FTC Act Section 5 is not a gray area.
Commodity content mills push high-volume output with no verification layer. No clinical fact-checking. No entity accuracy review. No Schema compliance.
In healthcare, that's not a quality problem. It's a liability.
The SEC has been explicit: accuracy and verifiability govern how AI-cited content is evaluated institutionally. A practice publishing unverified clinical content through a content mill isn't cutting costs — it's accumulating regulatory exposure while building nothing that earns a recommendation.
The content disappears. The risk stays.
How long does it take for AI Authority articles to start building measurable entity trust?
Authority doesn't run on a microwave schedule.
It builds in layers. Schema establishes the verified entity foundation first. Entity Signals confirm consistency across the practice's digital presence. Semantic Density compounds as each AI Authority article deepens coverage of a clinical territory.
There's no fixed timeline because every practice starts from a different baseline. What's consistent is the direction — every properly built AI Authority article added to the infrastructure moves the practice closer to the verdict.
Stop asking when you'll see results. Start asking how far behind you already are while the clock runs.
Can a healthcare practice retrofit its existing content library into AI Authority articles, or does everything need to be rebuilt from scratch?
Some content is worth rebuilding. Most is not. The audit is what tells you which is which.
Skip the audit and you end up retrofitting articles that were never going to earn a verdict — burning time and budget on content the engine will still ignore.
Content that already carries genuine clinical voice, accurate information, and real topical specificity has a structural foundation worth upgrading. Schema can be added. Entity Signals reinforced. Semantic Density expanded.
Content written purely for keyword placement — no clinical specificity, no authority signals — does not get retrofitted. It gets replaced.
Sentiment is not a decision framework. The audit is.
The Verdict Is Already Being Delivered — Is Your Name In It?
The courtroom framing was never a metaphor. It was a description.
Traditional search handed patients a list and asked them to choose. AI hands them a verdict.
That verdict is going out in your market right now. To the patients who typed their question into ChatGPT, Gemini, and Grok this morning.
The only question is whose name came back.
Schema anchors a practice to a verified entity. Entity signals confirm that authority claim holds across every platform AI checks. Semantic density gives the engine enough clinical depth to stake its recommendation on a name.
Gartner projects a 25% drop in traditional search volume by 2026. Not because patients stopped needing healthcare. Because they stopped tolerating a list when a verdict is one question away.
The practices that built authority infrastructure before that shift became irreversible are compounding. The ones that waited are invisible. And that gap is not closing — it widens every single month execution gets delayed.
This is not a content strategy. It is an authority asset — one that compounds with every AI Authority article added to the infrastructure, and one that decays the moment execution stops.
The AEO Content Strategy is the operational system. The diagnostic is the starting point. The practices that move before their market closes are the ones that get named.
AI engines do not hand patients options and wish them luck. They make a call. That call is going out in your market today. The only version of this story where your name is in it is the one where you built the infrastructure to earn it — a verdict, not a list.
AI is already naming someone in your market. Find out if it's you.
621 Enterprises, Inc. | Copyright 2026 | All rights reserved